https://www.panicaway.com/free-audio/?hop=flywait
Check More at https://htm101.com/track.php?c=cmlkPTgyNDk1MiZhaWQ9NjIyNTgxODI
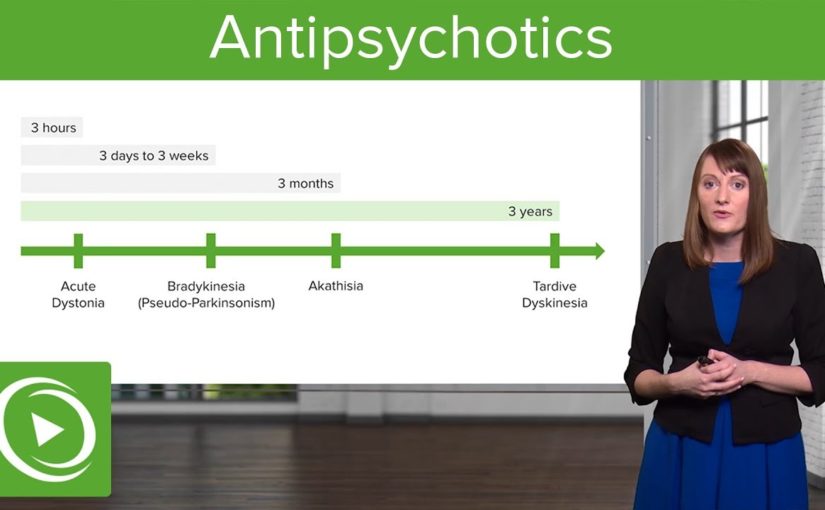
[ Music] antipsychotic therapy and pharmacology is an essential topic let’s go over the highlights here so antipsychotics are drugs also known as neuroleptics and they are categorized in terms of conventional and atypical they act by obstruct dopamine receptors and thereby reduce psychotic symptoms these are used to treat psychotic illness and too psychosis that starts along with other ailments so throughout the lecture serial you’ve learned that psychosis can actually appear as a evidence of severe depression it can also come up during times of dementia so there are a lot of uses for antipsychotics and they can occur in other patients who don’t merely have a primary psyche insane illnes as well so let’s go through the two types usual and atypical well a few examples of ordinary neuroleptics include chlorpromazine thyroid is een haloperidol a typical examples are things like risperidone and ziprasidone so the normal neuroleptics these are d2 dopamine antagonists they have a quite high authority now a normal neuroleptics do annoy dopamine however their lower authority for that and we are really too will target serotonin and histamine receptors as well the typical neuroleptics tend to be really good at analyse positive evidences but the atypicals are actually better at considering the negative evidences which we think of as the merits of the psychotic manifestations ordinary neuroleptics because of their dopamine siege they can really justification a great deal of extrapyramidal side effects that doesn’t happen just as much with the atypical neuroleptics nonetheless these are more likely to cause side effects like sedation and also weight gain or metabolic questions when it comes to the conventional neuroleptics there are again two subtypes there’s the high capacity normal neuroleptics and too low-toned capacity conventional neuroleptics so we’ll talk a little more about those last-minute and for the atypical Nora as I said before these tend to not only block dopamine but they likewise have a strong affinity for serotonin alpha receptors histamine receptors as well in serotonin so the antipsychotics basically again these target dopaminergic neurons that’s really the key and there are a few different dopamine pathways that you should be familiar with the nigrostriatal the Me’s a limbic and the tubero infundibular now neuroleptics are highly overweight soluble and therefore there are a lot of options for returning these intramuscularly or through an dose we’re gonna review that later but as a teaser it’s important to know that when it comes to taking an antipsychotic medication sometimes patients are very fomented in the hospital setting and it’s really nice to have the option to do an insertion of remedy likewise some people don’t like taking a pill every day and the longacting injectable antipsychotics actually allows users by monthly or monthly dosing which can be a nice option for cases so there are a lot of different squanders for antipsychotic prescriptions some are of course the primary psychotic diseases too mood conditions like mania and depression and Tourette’s disorder they can also be helpful there so let’s talk a little more about the conventional antipsychotics and let’s start with the low-pitched effectivenes wands so these have a little bit of a lower affinity for the dopamine receptor and patterns include cor promazine and thioridazine now there’s a higher incidence of anticholinergic influences with these remedies and a lower incidence of the extrapyramidal side effects that can be very upsetting to patients also a little of a lower incidence of neuroleptic malevolent syndrome which can be a deadly side effect of antipsychotic prescription the high capacity conventional antipsychotics have a very high affinity for dopamine siege and these include haloperidol flu phenazine and some other examples listed here there’s a very high incidence of EPS or extrapyramidal indications with these medications and also neuroleptic malignant illnes lower incidence of anticholinergic and antihistamine troubles so what are extrapyramidal side effects you might be wondering so it’s very important to know for your cards so extrapyramidal side effects come from dopamine blockade often through that nigrostriatal pathway and a very early ratifies of this can be acute dystonia now this might attest in your case as something like an oculogyric crisis where their seeings kind of roll up in their honcho it can also be seen as torticollis or next stiffness and acute dystonia can be very distressing to a patient and it can occur immediately or within hours next another eps evidences is brady kinesia or parkinsonian indications so this can look like masked facies where person doesn’t have a lot of expression it can also look like cogwheel rigidity which you might test for when you’re doing your physical exam on a patient some patients have this brady kinesia or hindered changes and they also can have a gate where they do something which is called turning on block meaning that they will make a sudden stop and then turn their entire body so it’s not very easy for them to shift and maneuver as it is for the rest of us they may also get a tremor which can be a cardinal peculiarity of a parkinsonian side effects from this prescription another difficulty that can occur within months of starting an antipsychotic medication is akathisia this is highly distressing to patients so what akathisia is is it’s an internal feel of restlessness it will often evident as a patient pacing perhap sounding their foot or their hand on their leg they’ll often describe to their doctor that they just feel like they want to crawl out of their surface so that’s a sign of a Cathie’s which again is very distressing and then a really important side effect of antipsychotics to be informed about is tardive dyskinesia now it can take times and even decades for a patient to develop tardive dyskinesia a little pearl for your quiz is that elderly Caucasian ladies her hat highest risk for developing tardive dyskinesia when they’re is dealing with an antipsychotic so what this actually looks like is abnormal shifts for example of somebody’s face you may see someone fastening their tongue out frequently or smacking their cheeks together this can also occur less frequently in boundaries or truncal areas and the really unfortunate thing about tardive dyskinesia is that in most cases it’s actually not reversible so it can be very permanent and a disfiguring side effects both traditional and atypical neuroleptics have similar efficacies in terms of treating positive indications of psychosis now you might remember the positive indications of psychosis or things like hallucinations hallucinations bizarre actions however when it comes to treating the negative symptoms of psychosis things like having a flat influence little motive good vigour speech alodia that’s better treated with one of the newer antipsychotics or atypical antipsychotics so the traditional antipsychotic side effects to review them are anti dopaminergic anti ham which we’ll go over that in more detail in a minute of course tardive dyskinesia and dystonia or in other words the EPS symptoms including brady kinesia and akathisia neuroleptic malignant illnes which we’ll talk about in more details too a serious side effect so in terms of tardive dyskinesia we spoke it before but another little pearl to know this is riding movements of the mouth and tongue when your patient is described as having that judge tardive dyskinesia the anti dopaminergic sideeffects is certainly the extrapyramidal symptoms too hyperprolactinemia and this is due to interference of dopamine in the tubero infundibular pathway so cases have been able to end up with so much dopamine blockade that they get a surge in prolactin and this can manifest is actually lactation from the breast and it can occur in women but also in men and then neuroleptic malevolent disorder is another extremely noteworthy sideeffect to look out for so I mention anti ham side effects before well let’s talk about that aims so that H is antihistamine where patients can become very sedated the a is anti alpha adrenergic side effects this can look like worth a static hypotension cardiac arrhythmias and sex dysfunction the anti muscarinic side effects include baked lip tachycardia urinary retention misty vision and constipation all things that are of course undesirable to your case they may also get force income promoted liver enzymes they may have eye difficulties or off the malla reasoning problems dermatological problems and seizures and because tardive dyskinesia is so incredibly important in a potentially irreversible and deforming side effects we’re mentioning it a good deal here it’s really important to be informed about for your quiz and it’s really important to note that it can lead to that permanent disfiguration if you have a patient showing signs of tardive dyskinesia you really want to consider lowering their dose of antipsychotic giving them a drug holiday from their antipsychotic or switching them to another worker preferably an atypical antipsychotic[ Music]

So here is the amazing thing about your ability, it’s made to rewire itself all the time. This is called neuroplasticity. Scientists believed that after childhoodour ability was pretty much locked in place, but now that we have better likeness technology, we are able to literally see how the brain deepens depending on how we use it. So, in this video I’m going to talk aboutone very simple thing you can do to rewire your brain to be less watchful, and it is simple, but it’s not easy.So I’m also going to share three steps youcan take to make it happen, and share ten extra skill you can develop on your own, orwith a therapist, to build up your ability to take control of your feeling. And if you would like to learn more in depthinformation about how analyse your nervousnes, I’ve got a course on Udemy that I am workingon called Rewiring the expectant brain, so you are able to check out that tie-in in the description. So, let’s start off with one example of neuroplasticity. In London the taxi moves have this superdifficult exam where they have to prepare by learn all of the streets and eventsand places in this huge city.Researchers took portraits of their ability beforethey started studying, and after this two year process and they only literally ableto see the brand-new neural connects, the wire that changed in the intelligence. And there’s good evidence that changing howyou think, like going to therapy, can actually change the structure of your psyche and thetypes of chemicals that it’s running out. Our brain has an amazing ability to rewireitself to learn, flourish, and mend. So, let’s talk about how to do that with tension. If we want to change how our brain processesanxiety, we need to understand three principles of anxiety. Number 1, we need to understand what is anxiety. Now, this may sound dumb, because you alreadyknow what anxiety feels like, but what you need to do is understand your perspectiveon anxiety. You need to let go of the relevant recommendations that anxietyis bad. Anxiety is not inherently bad. Anxiety is disagreeable, some times anxietyis illness, sometimes nervousnes does in accordance with the arrangements, but we all experience anxiety becauseit is supposed to serve a really important function.To motivate us to avoid real danger. We’re supposed to feel expectant when standingon a cliff hem, it helps us be safe. We’re supposed to feel desirous when we knowwe have an important test coming up because that should cause us to study. Anxiety tells us that something is importantto us. Anxiety and hullabaloo are basically the samechemical reaction in your organization with adrenaline triggering that affectionate activating andprepping you for action. When we look at anxiety as unpleasant, but acceptable and a regular part of life, unexpectedly we develop new tools to work withit, and that includes working with the other type of anxiety.So, the second thing we need to understandis we need to understand ailment distres. And this is when anxiety seems to take overyour life. This is anxiety that establishes it hard to go towork, to clas, or to enjoy life at all. And the harder you try to make it go away, the stronger and stronger it gets. Now, contrary to popular belief, that anxietyis agitation when it is more severe, anxiety is actually ailment when one of two thingshappen. When, number one, when you feel endanger whenyou are actually safe, and I made a video on this, it’s called perceived vs. actualsafety. For illustration I is cooperating with a patron who wasafraid of radiators. She would feel anxious and sweaty around themand she couldn’t represent herself go into a chamber with a radiator in it , now radiators are not actuallydangerous, but she was having a real, physiological response to something that was actually safe. So tension can be illness when you havea danger response in your form, but you are actually safe.The second mode feeling is likely to be disease is when your tension interferes with your ability to function. This is essentially what determines if youmeet the criteria for an anxiety disorder diagnosis. When your nervousnes, or your attempts to avoid anxiety stop you from effectively facing life. When this happens you start avoiding school, or calling in sick to work. You stop leaving the house, or spend timewith friends, pretty soon your feeling is taking over your life and stopping you fromdoing the things you desire. So causes talk about what causes anxiety to coiling out of control. This is called the anxiety cycle. Every day throughout our daytime “were having” events and we understand these experiences as either being safe or dangerous.So make say for example you determine a dog. Now, each person performs an experiencedifferently, for some people this would be extincting and fun, but for some reason youthink, that dog is going to bite me! This leads to feelings of horror, anxiety, maybeeven panic. These are unpleasant feelings and you may even make them as a clue that your thoughts are true. So, you escape, you run away, you get outtathere.And, Nothing bad happens. So your brain liberates this flood of easing, Whew! That was close! The only way I subsisted was because I ranaway. I could have died! And your intelligence judges I better do that again, I’m going to make make human avoid that situation by increasing their anxiety about it. And, vola! your nervousnes goes up. Every single time that we bypass a threat andsurvive, our mentality conceives, Let’s do that again. So it lays down neural pathways, this wiringthat reinforces that behavior. And the whole function of affections is to motivateus to action, but that’s a whole other video. So our mentality, because we have persuasion itthat the dog was a threat, it shall take such action into it’s own hands and it increases you anxietylevels around dogs.Every term we feel suspicion, and then avoidthe situation, our nervousnes height will go up a notch. So this is principle number three, avoidancefeeds illness suspicion. It literally originates devastating feeling. Now, there are lots of ways to avoid. There’s running away, and physically shunning, but there’s also feelings escape, so if you have social anxiety, you might still goto the party, but only if you get drunk ahead of time, or you might be in a relationship, but scared of getting hurt, so you don’t allow yourself to let the other person into yourheart.You stand emotionally remote, or you protectyour self by not dedicating. social media, rage, denounced, distraction, andeven coping sciences, can be avoidant. Regardless of the type of avoidance, it increasesyour nervousnes and, all the more serious, it reduces down your world. So with the dog example, you might start avoiding situations where a puppy might be present, by not going to friend’s homes, or bouncing thepark. And your world contracts, you miss out on goodrelationships, or you stop going to parties.And your world gets more and more restricted. Avoidance can perform your world tiny and scaryand happy. But each time you get anxious and eschewed something, and live, your psyche multiplies your nervousnes in that area. Now, looking at this cycles/second, “were having” two placeswhere we can intervene. Where we can stop that anxiety from spiralingout of control. The first place is with our actions.When we feel suspicion, but we are actuallysafe, if we stick with it, if we stay there, we experience our ardours and sensationswith out running away, and again, if you do this, and you don’t die, then your psyche learnswhew! what a comfort! I guess that not all pups are dangerous, let’sdo that again! And it sends out a surge of succour. This leads to a gradual decrease in anxietyover time, and a gradual increase in your feelings muscles, your ability to feel sentiments and impressions that are unpleasant, with out needing to escape them all the time. So you to be all right at feeling. As you do this your brain literally lays downnew neuro pathways saying not all bird-dogs are dangerous, I don’t need to be anxious arounddogs. And it literally changes your brain chemistry, liberating less cortisol and adrenaline and other stress hormones.This is the most straight forward way torewire your psyche to have little nervousnes. But, I get it, this is super hard-boiled. If “its been” easy, you would have already doneit. So I’m going to break it down into three bigsteps for you. Now on a line-up greenback, the second place in thiscycle to intervene is with your thoughts. Changing how you think about the dog. And this can be a potent and efficient treatmenttoo, but it can also get really complicated. And it is more efficient before your expectant, ratherthan during. Now I can talk about some of the ways youcan change your thinking in other videos, but in this video we’re going to talk abouthe most straight forward way to rewire your expectant intelligence and that’s through your wars. So, how to get it on. There are three steps. So step one, make an exposure hierarchy, I’ve made and entire video about this, but mostly you take one thing that scares you and youbreak it down into teeny minuscule paces, and you start by courageously facing the easiest onefirst.Now this is the part that most people miss. They jump in too fast and then they panicor the flee and they never make love again, and then that fright is reinforced. So make and exposure hierarchy and write downas countless teeny little steps as you can think of. Step two, deepen your rules. Now, spirit doesn’t mean the absence of fear, but preferring that something is more important that by-passing panic. In acceptance and commitment therapy, thisis called willingness. Allowing yourself to do something even thoughit makes you awkward. If you make a rule for your ego like, I’mgoing to do this until I get too watchful, then you brain will be like cool, let’s dothat, then I can escape. So it will constitute you really anxious, and whenwe say I’m going to do this thing unless in reaches me desirous, then we are just invitinganxiety to make all of our decisions for us. So when it comes to exposure, you choose aneasier activity to start with and then you stay with it and watch yourself for a certainamount of time, or until your nervousnes increases by half during the exposure.Now, while you’re facing your nervousnes andpracticing your willingness, footing works, and selfregulation activities, this bodyupapproach to weakening feeling can be useful. But the most important part is that you sitwith your feeling for a little while until it declines, or at least for a certain setamount of duration. Now, step three. Do it. Face it. Go get anxious and see if you live. A little spoiler alerting here, you will. So with the dog example, start be repeatedlyimagining yourself interacting with a pup and you rule every day for ten minutesuntil that activity no longer originates you very anxious.And then you might want to work with a friendwho has a dog to set up the nest paces. So you might check a hound through a window andjust stay there and you sit with it and you breath with it and you allow your self torelax and you do this every day for ten minutes until your nervousnes reduces. And then you pattern being in the same roomwith a insignificant puppy on a leash, and the perhaps touching a tiny dog on a leash and then pettinga tiny dog on a leash and eventually you are moving up to a bigger dog and the off a leashthen eventually you get your self to the point where you can go to a pup common, sit down, and stay there for thirty minutes. It’s ok it you feel uneasy. It’s ok if you feel uncomfortable or you sweat, or you shake, or whatever, but you time stick with it. And pretty soon your mentality learns It’s cool, most pups are safe, your ok. And your feeling will decrease. Now again, you can do some physiological groundingactivities while in the midst of your suspicion, but don’t use those as another way to justavoid anxiety.Use those as a highway to practise willingness. This willingness to feel what you are feelingand professed it as being regular, natural and ok. So there’s the simple solution to anxiety. face your suspicions and they will decrease. This may seem too simple, or too absurd, too big of a bounce, so therapist have organized a assortment of ways to break that leap down intoa knot of tiny paces, a bunch of talents that you are eligible to learn to make it easier. If you want to go more in depth into thatlet’s do that. Let’s talk about the more detailed processof how we do this. The specific skills that help us move fromanxiety avoidance to ability over our nervousnes. Because I am trying to cram so much informationinto this topic, I’ve decided to split this video up in to two parts. So check out part two for the ten knowledge youcan develop to help you face your nervousness. Gradual exposure therapy, which is what Ijust described, is a researched backed approached demonstrate to help reduce anxiety and plow anxietydisorders.It does this because it literally changesthe mentality. Rewiring the neuro pathways and changing therelease of substances in the brain. So make sure to check out my part two withthose ten talents to assist you face your frights and if you’d like to learn more in depth informationabout how to treat you anxiety, I’ve got a course on Udemy that I am working on it’scall Rewiring the Anxious Brain, so you can also check out that associate in the description. Now, please share this video, you never know who might benefit from it, thank you for having watching and take care ..

So today we’re talking about sensoryprocessing ill and suspicion and which comes first.Is it sometimes that we get anxious and therefore we become sensory reactive andsuper sensitive or under energized or is it that our sensory causes theproblem and this is a really good question and it’s a really important oneto address well so we’re really just going to introduce some of the conceptsjust now and generating some things into the room that we need to think aboutwe’re not going to solve all the problems that the issue fetches upbecause that would take days.So let’s give it a go from anoccupational care position when we think about sensory processing disorderand anxiety we’re really starting to wonder if the distress that our client is carrying is really secondary to the sensory processing disorder thechallenges that that generates and so that’s really where I’m going to speakto today and we will bring in a psychologistlater to talk about when feeling is the primary part of the picture and more ofthe root cause of what’s going on. So if we think about the sensory systems andreally try and unpack them and go deep with what it might mean to have adysfunction in one or many of them then we can start to understand that it wouldnaturally be a cause of nervousnes because fluctuation needs to be organized and underour assure to feel safe our sensory structures have a awfully primitive functionof impeding us alive as well as helping us to move, move beautifully, move withfinesse, navigate gaps and become social creatures.The firstly patch though is this safety keeping us aliveOur sense of balance, our vestibular sense that spirit level ofliquid in the inner ear and quartzs that tells us if we’re upright againstgravity or where we are that method, its first part is to keep us aliveand if we get turned upside down real quickit’s gonna make all the alarms go off and it’s going to be telling us that weneed to change something pretty quick so we go into a regime of flight or into astate of push or even more serious into a freeze district when this system sendsall the alarms off.Also when the system isn’t getting enough informationit starts to wonder if I’m safe and alarm systems, alarm bells start to ring.So for example if you’ve ever been in an elevator and there’s that time beforeyou can really tell if you’re moving yet or not, there’s that instant andpeople start to look at each other like are we okay? what’s about to happen here? because we’re not had enough data sufficient information from our vestibularsystem to really assess if we’re safe, if the situation is okay which course we’removing. And again that sense of frighten that you get when you’re on a publictransport, maybe a bus and the bus next to you which one’s moving is it me orthe bus next to me? My visual arrangement and my vestibular arrangement are in conflict andI can’t tell what’s going on, I go into alarm.So these are just examplestrying to help us empathize with individuals who struggle with theirvestibular information on a daytoday basis and that state of deepened fright, arousal that they get into or that they exist in for most of the day, which wouldlook like an anxiety disorder but it’s not it’s not clinical nervousnes in thosesituations, it’s anxiety that’s caused by a lack of integration of the vestibular arrangement with perhaps other organisations contesting report , not enoughinformation and being too quickly and too often in a state of oppose or flight orfreeze.The same falls for our position sense our proprioceptors which arepredominantly in our joints and when we get compression or when we get tractionon our seams we know where we are in space. I often would fall asleep on myarm and go to that level past pins and needles when my limb is just like is iteven there ?! and that if you’ve ever known that is really alarming, thealarm systems go off and your mas starts to say this is not okay, I’ve losta whole limb here and you know what’s happened is that there’s that blood flowhas been a problem, the proprioceptors aren’t serving very well.Your senseof proprioception maintains you fastened and grinded in your own body and when thatsystem is inaccurate, it’s inconsistent, it’s not giving you greatinformation then your arousal goes up and you start to have alarm bells goingoff in your lower mentality saying I’m not safe, I need to be wary, I need to orientto everything that’s going on around me and that inspects again that caution, thatanxiety.But it’s got a sensory root in these cases, but we don’t call theseanxiety agitations, we’re visit that a response to what’s going on with thesensory systems and we could go on with speciman after speciman. A reallyimportant one to think about is the child who really has trouble withmultiple sensory organisations at once and the most challenging environment for thatchild generally speaking is institution because the school environment isloud, it has buzzers, it has visual jumble, there are things hanging from theceiling, there are Mobile’s, there are still posters, there’s Halloween presentations, there’s resembles in the cafeteria, children are entirely unpredictable and they slap you andthey push you and your nervous system is constantly vigilantly trying to keep youalive and you looks just like a uneasy child an vigorous child a child withbehaviors but it comes back down to sensory processing. So this is wherewe start to say with some of our children is the sensory or is thisanxiety? When this child’s at clas they cannot coping, their patience for stressis minimal because they’re using all their resources just to get through theday, or are they so stressed that they’re reactive and we need to figure out whichone comes first.And some of these children where the multisensory piece isthe problematic piece so what we do with those minors is we increase as much stressas possible, we cater to their sensory systems, we nourish their sensory plans, we settled them in the claim regiman, we look at the other accentuates in their life arethey getting enough sleep? Are they imbibing enough water? Are they eatingenough food? How are their relationships? How is their timetable? How are theygetting to school? What’s their socioeconomic status? All of thesestresses we look what i found, we nourish the sensory systems and then we wait and wewatch and we start to unpack.And if this child is able to adapt better when wenourish their sensory systems and adapt the environment, then we know thatfundamentally what’s going on here is not anxiety but that the sensorystresses are so great that they’re causing an anxiety response. But if afteradapting and treating for sensory the suspicion is still particularly prevailing then werefer we find a really good mental health provider who are familiar with sensory but we refer to them and we get them involved and we start unpacking the restof the picture and what’s going on and that’s really important. So that’s been alittle introduction to sensory processing disorder and nervousnes and theinteractions between the two. It’s sensory awareness month. I’m VirginiaSpielmann the associate chairman of STAR Institute now and weare trying to raise awareness, educate and research more into sensoryprocessing ailments so there will be a link that we’d love you to click on toshow your subsistence. Please share, note and give us know what you want todiscuss ..

Sarah queries How can I stop my panicattacks naturally? Im interested in mindfulness meditation and Im wondering, does it work for panic attacks? Hi, Im Michael Norman and welcome to PanicFree TV Q& A. This is where as research scientists and anxiety professional, I answer your most pressingquestions about how to quickly stop your panic attacks for good so that you can enjoya normal, panicfree life again. Okay, so there are two questions now: One is about how to stop panic attacks naturally. The other is about mindfulness meditation, exclusively. Gives talk about mindfulness first. Now, the research clearly shows that mindfulnesscan help with panic attacks, but its not for everyone. I’ll interpret more in precisely amoment but firstly let me take 30 seconds and quickly explain what mindfulness is, foranyone who doesnt know. One of my current definitions of mindfulnessis that its purposely bringing your full attention to the present moment, really observingand accepting whatever is happening in your current experience, without approximate it atall.Now, this is just one definition, and definitionsare always merely Aims to describe reality. If you was just going to a eatery and you merely readthe menu that would never supplant actually smacking the nutrient, and so the only true wayto know what mindfulness is like for you, was an attempt it. This can be done formally with a mediationpractice whatever it is you dedicate blocks of time to practicing being fully present, aware andaccepting of some aspect of your current experience, like your breathing. It can alsobe done informally throughout the day, simply by being PRESENT to your senses, to whateveryou happen to be doing. So how does mindfulness relate to stoppinga panic attack? Well if you’ve already watched my freePanic Free TV foundation serials then you already know thatone of the main thingsthat oils a panic attack is trying to fight it Mindfulness offers us one antidote thatof being present to, and learning toACCEPT rather than fight, whatever desirous thoughtsor body sensations that you might be experiencing.While it doesn’t immediately stop a panicattack, if you can accept and precisely be present with a panic attack, that takes away the fuelthat restrains that panic attack proceeding. As mindfulness explorer Jon KabatZinn introduces it the mindfulnessattitude is You CANT stop the brandishes, but you CAN learn to channel-surf. Now, apparently perfectly abiding a panic attackis FAR, FAR easier said than done … which is why it makes so much practice. This is reflected in the two mindfulnessbasedprograms that have been show scientifically to help with panic attacks. Theyre both 8 week planneds they both involveup to 30 hours of group instruction plus this relates to 45 minutes to an hour of meditationpractice, each day by yourself. Now, if youre thinking that this is a hugeinvestment of day, then I definitely concur. If you JUST want to end your panic attacksthen, for me, its obviously not worth it. I demonstrated in you far faster, far more reliableand far more effective ways of turn panicfree. But if youre already interested in meditation, and if youre previously considering starting your own daily rehearse then definitelydo it because there is a huge amount of research showing that mindfulness can help reduce stress, dwell, recession, even back pain, and it can increase your general sense of wellbeing.And when it comes to panic even though we need a lot more research it seems tohelp about 75% of parties over such courses of a year IF theyre willing to invest thetime into a daily mindfulness practice.Now onto the second question: whats thebest approaching to stop panic attacks naturally? Well, this is exactly what I cover this indetail in my free Panic Free TV foundation sequences Its simple sciencebased help forpanic attacks that will show you the fastest, natural direction to go from wherever you areright now back to a life thats as regular, carefree, and panicfree, as anyone elseyou know. The solutions for panic is simple, buttheyre passionately counterintuitive and thats why I initiated this footing line. Again, its totally free, it will makean immediate, important difference in their own lives and to watch it right now, simplyclick on the link on your screen or in the specific characteristics below, enter your details, and get started today on your outing back to a regular, panicfree life Im Michael Norman.Thank you so much better forwatching. Ill see you soon ..

Sometimes it can be easy to find a trigger.For speciman, people with a specific phobia of something can have anxiety when they seethat special object. In some clients, it’s much harder to find a prompt. Panic attacks, for instance, can come out of the blue without any self-evident initiation. Sometimes, people can also experience anticipatory anxiety, so they feel anxious even before they’re in a placewhere they are stressed. In status such as PTSD( posttraumatic stress malady) distres can start after people witness something that prompts them of the past agonizing event.This meaning that the damage has not been fully processed and still feigns people. It’s important to remember that sometimes you can manage anxiety by avoiding the initiations. So, escape establishes it harder to identify a particular trigger ..
Hello, I’m Norman Swan. Welcome to this programon maintaining wellbeing, dimple and tension in workers withprostate cancer, and their development partners. Prostate cancer is the most commoncancer in Australian boys apart from nonmelanotic skin cancer. One in nine will develop the illnessin their lifetime. Men with prostate cancerreport higher levels of depression than the general community, but the rate of depression and anxietyin their partners is even greater more than double the incidenceof the Australian parish. Psychological distress and depressionin humankinds with prostate cancer, and their partners, is often overlookedand underdiagnosed. There’s a fair fragment of evidencethat cancerassociated depression has its own problems, and that’s what we’ll explore. You’ll find useful resources available on the Rural Health EducationFoundation’s website: You’re can’t go there yetbecause you’ve got to meet our panel.Suzanne Chambers is director of researchof the Cancer Council Queensland and professor of psychooncologyat Griffith University. Welcome, Suzanne. Thank You, Norman. Suzanne is a member of theAustralian Cancer Network Working Party for the developmentof Clinical Practice Guidelines for the Managementof Advanced Prostate Cancer. As you’ll hear, that’s associated withsignificant psychological morbidity. Caroline Johnsonis a general practitioner and lecturerat the University of Melbourne. Welcome, Caroline. Thanks. Caroline is about to complete her PhD on monitoring depressionin general practice. Peter Strange is a nurse practitionerspecialising in mens health within the agricultural Bendigo area. Welcome, Peter. Good evening. NORMAN: You do portable clinics? We go to workplaces and areas where there aren’t physicians. What sort of things do you do? Health ratings for men. In particular, we look at preventative remedy, getting to the guysthat won’t come and see their doctors. NORMAN: You’re involved inthe Men’s Shed movement? Yeah. Anywhere we can get to menfor preventativetype health. NORMAN: Getting close to too much information. Colin Bartlettis a prostate cancer survivor, and also suffered depressionthrough his illness, as you’ll hear.He’s facilitator for the WestmeadHospital Prostate Cancer Support Group in Sydney, and is heavily involvedin the Prostate Cancer Foundation. Welcome, Colin. Good evening. Therefore welcomed you all. Colin, tell me your floor. I was asked to have a PSA testby my doctor, under protest, I was. Had it done. Four days later, he says, we have a problem I had the problem. Go to a urologist. I was given a DRE, and instantly told, there’s an irregularity.We’re going to have togo to another theatre. At that time, it didn’t reallycome home, but the next bit did. NORMAN: You didn’t realise you wereon a truck scooting towards the wall? No, I didn’t. I then went to have a biopsy done. It was after the biopsythat all countries of the world hurtled. That was when Trish was with me, my partner, and Andrew precisely told us straightaway, you have cancer.What are you going to do about it? Shock, repugnance. I anticipate she was more devastatedthan I was. The thinker just goes into freefall what am I going to do now? Do you retain the emotionattached to that? The feeling is one of mistrust why me? Why is this happening to me? A little bit of sect are entered into it, because I turning now to him and said, I’m going to make sure other lovers don’t fall into the same trapthat I’ve fallen into.That’s all I could say at that place. So you were offered a series of options? Yes, I was given three alternatives, exactly given them straight out a radical prostatectomy, radiation therapy or we could possibly go onto some therapy if it suited. It was just left at that, and I was to manufacture the choice. NORMAN: How did you construct the choice? Seeing as the urologistwasn’t much aid, I did get a piece of paper that indicated a prostate cancersupport group at Westmead Hospital. I observed the guy who was the facilitator, who still is, by the way. He gave me some informationabout selects. I went to see him, and we spoke it. We decided really “they dont have” optionbut a progressive prostatectomy because the Gleason score was high 7. The PSA was 20. It meantI actually had nowhere else to go. When did the depression hit? That, Norman, is an unknown factor. I don’t really know when it truly smacked, but it’s been an insidious thing that’sbeen growing and growing and developing. Possibly, it really came homeprobably three to four months after everything, I recalled, had colonized down. It hadn’t. So you had the operation.How did it leave you? I felt pretty good, actually.I wasn’t especially annoyed. I didn’t have any hurting or anything. I was still in this freefall what am I going to do now? I didn’t really knowwhat I was going to do.Didn’t know what to expect either. Were you feeling anxiety? I was anxious, of course I was, very anxious abouthow Trish was feeling. She was my main concern. NORMAN: How was it travelling between you? Then? Very good. We were pretty good. We’d suffered a few other questions whichhad brought us a bit closer together. So we were in a propitiou positionat that stagecoach, but it unwound later on. NORMAN: Unwound? I’m afraid I was the onewho was the problem because I virtually shut off. What you feel is pain, and it’s a mental pain. How do you run away from it, get away from it? I attained solace in getting on my bicycle and going off and doing three or fourhours’ go and coming home. NORMAN: The male thingof journeying off into the sunset? Virtually, yes. Into the sunrise, actually, at that time of day when I’m around.You sort of get yourselfinto your own little sphere, into your own little bubble. She wasn’t ableto make contact with you? We didn’t talk much about it , no. I had a lot of men come to talk to me. I had a lot of supportfrom the aid group itself. It more or less articulated her out on a limb. She really didn’t do muchin that course at all. How did it get better? I think it got better formerly we hadgot rid of the continence trouble. I suffered a postoperative hernia, and “were having” that specified. After that, things startedto get back into a normal operation but for one thing I had continencetroubles. I had incontinence. It wasn’t bad, but it was enoughto cause us some concern. And erectional purpose had also gone. Did anybody recognise the depression? No. That’s the unspeakable thing about it. I never talked to anyone, andI didn’t see what was happening to me.I didn’t know what was happening to me. How did the depressionshow itself in you? The dip demo probablyafter about three to four years. I began to get terribly edgy, extremely petulant, and being a bit picky with Trish. I look back at it, I’m ashamedof some of the things I told us to her, like, I don’t have to drive with you, do I? I was beginning to get very criticalabout her driving the car. I didn’t notice it.I was just picked up as a sulky old man who’d had a prostate operation. NORMAN: Were you sleeping? No , not very well at all. NORMAN: Had you lost interestin things around you? Yes, altogether. Had you thought of killing yourself? No, that didn’t come into it. There’s no selfharm in me. I’m very firm about that.There’s no selfharm.But you intent upnot get given for it? Quite a long time. In fact, it’s only aftersix years of going through this that I lastly was recognisedas having a problem. That was going to a Men’s Shed function and listening to somebodytalk about depression. His recommendation was then, go and talk to your GP. You do have a good one? Yes, I do.I’ve known him for 20 times. He said, he will be the best personto see. He knows a good deal about you. When I did go to Jim, he said, more orless, I’ve been waiting for you to come. NORMAN: But hadn’t asked? But hadn’t asked. In a nature, that’s a bit disappointing, but I won’t hold it against him. Certainly, we’re on the right track now.We have found the direction through. We’re having a good life. There’s been a spinoff. I’ve been ontomedication, and it’s quite a new floor. The medication, I started in September’ 09 and by December’ 09, I’m beginning to say, where’s this continence problem gone? NORMAN: Things have been fixed in one affect? It’s just gone.I’m the same as you would be, the same as any manwho has not had a prostatectomy.Which is quite surprising. Asking then a beyondblue personwhat had happened, she said straightaway, what drug are you on? It’s a serotonin type of medication. She said, are you thinking about it anymore? And I said , no.Really, I hadn’t really thought about it. She said, stress continence. It’s gone. Peter, you’re nod sagely there. This is obviously not an singular storyfor you. No. I’m very interested in your narration, peculiarly connecting withthe act of uncovering for early diagnosis of depressionwas at Men In Sheds.Well, it wasn’t early five, six years. True. The firstly diagnosis. It’s interesting that parish groupsand support groups and people you just have a chat tooften will pick up these things. It’s really important, a point to get across from the word go, that clinicians need to ask how people are travelling, if it’s as simple as that. That’s probably what you needed, Colin, for someone to situated their nose in and give him an opportunity to listen. You’ll consider menwith psychological issues, especially hollow and distres, a lot. Is it different when males have cancer, and is it differentwhen adults have prostate cancer? I think it is. Perhaps the more extreme the morbidityor the condition … Sometimes I study guys implant it moreso it’s even harder to get out.It does become more extreme. NORMAN: When you say more extreme, you signify what? The movement of the depression. The medical plight and how theyperceive it will determine that. That’s important.If we can help them through, give them education and explanation, perhaps we can lessen that. The waiting game waiting for research. Too, it encroaches with your senseof your own masculinity. Absolutely. Men will hasten onward. We might start, as medical professionals, saying, we’re having a PSA test.This may not mean anything. Some humankinds will automatically race aheadright to I’m going to have cancer, male erecticle dysfunction, wedlock problemsand all those things. As clinicians, we need to think aboutthat and cure that we are able to. It may not be unrealistic.PETER: I agree. Caroline, a familiar storyfrom your point of view as a general practitionerinterested in depression? It is indeed. One of the biggest ploys for GPsis getting this balance between the physicaland the psychological.If someone comes inwith a cancer diagnosis, we expect, probably rightly, that the most difficult thing on their mind is, is this going to kill me? So we focus on the physical. We often “re saying”, how are you touring? How’s it going? How are you coping? We think that’s usscreening for sadnes, but patients often think we’re saying, how are you coping with the cancer? You’re right, we have to bemore specific with questions. NORMAN: More systematic? That’s an interesting point. There aren’t countless experiment trialsthat show that by introducingsystematic screening … You might pick up more casesof hollow but whether you’ll get better outcomesis controversial unless you actually do something. Hard to get better outcomes unless youfind out somebody who’s got depression. In the late’ 90 s, there were lots of studies that showed that if “youre asking” beings, are you chilled, and they say yes, it doesn’t necessarily meananything will to get out of here. It’s important to emphasise thatif you ask the question, you need some kind of planof what to do next.Suzanne, how could it have been different? The first thing I would say is thatthe narration we heard is very typical to seeing how people often present whenthey’re distressed and have recession, for example, after cancer being withdrawn, annoyed, a strain on the relationship. It does get put down to beinga cranky old man, which is quite untrue. We know there’s a range of risk factorspredictive of someone more likely to suffer distress. What are they? Things like lower levels of education, being inadequate, having a previous psychiatric or autobiography of recession is important. Stage of disease and symptomatologycan be important as well. But the only thing, if you measureat diagnosis the level of distress, that’s the biggest predictorof subsequent distress. If someone had deterred a close gaze on yourlevels of distress from the beginning, they probably would have picked upthat they were high, and get in early. In essence, you had a prolonged periodof suffering that was unnecessary. Those are times you can’t get back. Yes. You’ve done well, and that’s great, but it’s not a good thing thatthat went on for so long.The other thing is, if you think about it, there are three main components to thinkabout with a cancerspecific distress. There’s the psychological aspect the distress the man exhibitswhether he’s depressed or agitated, having obtrusive concludes. Then there’s the social situation what’shis relationship like with his partner? Is that a supportive affair? Has it been there for a long time? Is it a well of resource for him? The third is, what’s happened with the cancer? How has the care wreaked? What’s the manifestation sketch like? When treating a cancerrelated distress, you’ve got to treat all those. Very important that you too considered side effects and symptomsof the cancer treatment.Otherwise, the interventiondoesn’t looking relevant to the man, who’s mainly marking I’ve gotcancer as his presenting problem. One of the greatest problemsthat we face within the support group is one of continence. Incontinence is a big problem. To a degree, a great deal of people don’tnotice or recognise it. We’re focusing on it at the moment to impart a little bit of awarenessto the people in the funding group to know that there is something thereto help them. A heap of them suffer greatlywith continence troubles. And it’s pretty depressing.COLIN: Very much. Which is your point. Exactly right. You can’t divorce those physical thingsfrom the psychological bang. When they do unmet encouraging caresurveys of men with prostate cancer, the big ones areunmet psychological needs with regards tofear of cancer appearance, and unmet sexuality needs.If I were going to pick something, I’d focus on those two sides for men who are surviving prostate cancer. Do you think you’ve got the equipmentto ask the questions, Caroline? For mental things? NORMAN: To explore this. Everybody has a different form. If you make it one of the purposes of your routinepractice to raise the issue … We know that whenyou have a serious illness, it is possible psychologically distressing. These are questions I’m going to ask, is it OK with you? So people knowyou’re not lope through a checklist. So afford us the write that you…It’s often useful for GPsto hear the script that professionals use. What are some of the questionsyou might feel tricky about? The screening toolsthat we use as psychologists are a little different to what worksin general practice. I’ll say what I would do, then I’ll defer to Caroline. We commonly usethe distress thermometer, a single entry. I’ll say, I’m going to ask youa question that musics a little strange to check that I understand whereyou’re at and I’m not missing anything.On a scale from 0 to 10, where 10 is really high-pitched distressand 0 is I’m fine … NORMAN: You “use the worddistress” ?’ I use the word ‘distress .’ .. where would you see yourself? They’ll give me a number. If it’s lessthan 4, I think they’re doing OK. If it’s over 4 or 5, there’s a good chancethey’ve got anxiety or dimple. If it’s over 7 or 8, I’m concerned by them. That cures guidebook how muchI will go indepth with such person or persons about their psychological condition. What I always do is cause a personset their agenda first with me by saying, tell me what’s been happening to you, why you’ve come to meand what you’d like help with. Then weave it into the conversation. NORMAN: That’s in referral situation, whereas a GP is in the first situation.I heard that technique precisely tonight, and I think it’s great. We do it all the time with hurting. We say, on a scale of 0 to 10, where would you rate this agony? It reaches perfect feel to do that. It is a nonlabelled wayof parent distress. NORMAN: And it’s a clairvoyant thing. Right. If we’re talking specific aboutdepression, I still make questions are good in the last two weeks or month, have youbeen feeling down most of the the time? Have you lost interest in pleasure? Researchers in New Zealand did a trialwhere they added the question would you like is contributing to that? No, yes or yes but not today.They found that extra questionwas a good way of picking up on people that might have been a false positive. If you ask people, would you like aid, and they say yes, it should ring a bellthat you should focus on them. Could something have been doneat the diagnostic place? For pattern, one of the very best predictors of whether or notyou’ll regain erectile function is how much erectile functionyou had before, regardless of your age. Could things have been donewith Colin earlier? Is there any evidence of preventability? There is evidence of preventability. What’s important is that at the outsetpeople understand this is going to bepsychologically tough. It substantiates them. If you start feelingdistressed, you’re not saying, I’m weak.It’s saying, this is a tough experience.Let me give you some tips-off about things to do to help yourself. Ideally, you work with the manand his partner. The best thing to do isget them working as a unit and preempt relationship publishes, which are not uncommonafter a diagnosis of prostate cancer. Research in South Australia showed that much as mortals don’t likeexpressing their distress, gals don’t like conveying it either’ cause they feel they have tobe the rock in this time of disturbance. Maidens are often the feelings spongein a relationship. They take responsibilityfor maintaining emotional poise, and they suck everything is up. So, while you’re getting cranky, she’s sucking it up, feeling worse. Often, men and women havedifferent communication structures about dealing with difficulties. If you can help them negotiate a wayto help them do that, that helps each person feel validated.It’s important that people knowtough times are ahead, and that they give a hint of, if you start feeling this wayand it goes on … It’s normal to feel distress, but if this goes on for some time , no stamps for mettle. Go back and see your GP or summon person, and be helped early. NORMAN: Peter? We may need to ask more than formerly. We may be asking someone like Colinhow he’s going, how he’s feeling, and at that stage of the process and this is stretched out over fiveor six years he may be doing well, so we need to keep asking himhow he’s roam and questioning those important questions.There will be periodswhen he goes up and down. How important do you think settingexpectations is at the beginning so people know the journey they’re on? We need to be very honest. We need to keep it very simplebecause men that are having accentuates won’t be ableto take in a lot of information. So we need to be very honest. We can’t prophesy what’s going to happen, but these are the possibilities. Colin, in retrospect, what do you thinkcould have been done for you at that diagnostic place, before anyonehad laid a hand or spear on you, that would have made a difference? One of the thingsthat would make a difference is having what we call a road maplaid down of what’s going to be, what the high expectations are, what’s going to happen.NORMAN: Physically and psychologically? Yes. The psychological onewould have been very important because I didn’t realisethat was going to happen. That’s been the most devastating proportion, is the mental persona. We’re sort of out of it, but it’s stilldevastating, the mental chip. In country towns, it is going tobe the GP who will carry the burden. That’s true. There are more openings nowfor GPs to get subscribe, but it is harder in the agricultural position because there are lesshealth professionals.It’s great that there arenurse practitioners now. Some practises have mentalhealth nursesthat can help, specially parties withmore serious psychiatric illness. There’s also dial support for GPsthrough GP Psych Support. But, eventually, the GP is often seeingboth partners in a relationship, so they often get the warning signsearlier. Knowing how to act on thatis the challenge.Suzanne, as the pilgrimage progresses? Things like hormone treatmentcan be pretty rough psychologically. That’s right. It’s importantto recognise it is a journey. Stress is typically very highat diagnosis, generally quite rapidly lessens, thencan spike when critical happens happen, for example, a cancer occurrence, where distress can be higherthan at initial diagnosis. If a man is diagnosed withrecurrent cancer, he’s at some extent going to be put ontohormone treatment.Hormone treatmentshave serious side effects such as mood disturbance, cognitivechanges, changes in muscle mass, central adiposity, osteoporosis. NORMAN: Libido disappearing. Libido remains, male erecticle dysfunction. There’s good work being done in WesternAustralia abusing highintensity exercise to help with that. There are things that can be donethat are complimentary rehabilitations. Serious exercising, physiology office, and there’s Medicare rebates for that exercise physiology under certain schemes. Again, for the GP, it’s being awarethat things change over time for men.Every age you insure themis an opportunity to check how things arewith the prostate cancer. Let’s go to our case studyand work through some of these issues. Don is a 52 yearold farmer. He comes to you, Caroline, with urinary symptoms. When you do a digital interrogation, it feels a little peculiar, and his PSA comes back at 7. You cite him for a biopsy because his brother was diagnosed with prostate cancer, which is why you did the PSA and DRE. He was widowed four years earlier, and got a bit chilled. His wife died of breast cancer after many years of illness. Luckily, he’s recently repartnered. Caroline, what’s your approaching going to be towards Don? He’s got the risk factors. He does. First of all, any time you do a test for cancer, you should try and discusswith the person or persons before you do the test what the possible sequels “wouldve been”, because you don’t want to read someoneand say, the test is abnormal, and them getting terribly distressedand panicking before they listen what it actually means.I try and tell people beforehandthe possible outcomes without going into detail. Then when the test comes back andthere is concern this could be cancer, taking into account his determining factor, past history. He’s also had knowledge of cancerthrough two brothers and his wife. That might reform his perceptionof what that is likely to represent. He has existing lore, but it may be helpful or unhelpful. You might want to knowwhat happened to his brother to see what making he’s got. Perfectly. It will be significant. The buzzer should be ringing straightaway when you’re presented withthat sort of history. Start asking questions about his brotherand how he feels and how much that’s feigned him. That’s going to drive him intothat provision, perhaps, of recession. Suzanne, is there anything you can doat this point to steelbelt him, apart from improvinghis mental substitutes? The things I’ve already mentionedare appropriate for this person. I suspect, close surveillance. Like Peter said, catch out what slide he has in his head about whatprostate cancer diagnosis intends. It may be he’s more focused onwhat happened to his wife she died a difficult demise, and that might happen to me.Or it could be focused onwhat happened to his brother. You don’t knowuntil you ask those questions. If he’s got position creeds about cancerthat are unhelpful or mistaken, you can try and correct those. Just remain a close racetrack on him. He’s in a new rapport, so he doesn’t have a 25 year history of coping together through adversity. That marry, I would anticipatethey would need backing and perhapssome liaison adviser. This is going to be a tough experience.It happens to you as a pair. Talk about things you can doto support each other through it. The fact that he’s gotthe history of depression, it rings buzzers thathe’s more at risk of recession again. You can use that to your advantage what was it like last meter? What were the symptoms you knowledge? What would you do if you did a screeningand detected he was chilled? I would askwhat worked for him last time.If he had antidepressantsand they were very effective and he had same manifestations this time, I’d have no hesitationthat he try it again. Suzanne, the evidence is that antidepressantsdon’t make a lot of difference at the slight to moderateend of the scale of assessments and that cognitive behavioural therapywill improve their resilience. The only thingthat improves your resilience in reducing recurrenceis psychotherapy. I don’t knowthat I is in favour of that. A combined coming is appropriateand separately accommodated. You can look at studies, then you look at people. I’m with Caroline what did he do that worked last age? I think that trying to help peopledevelop adaptive coping programmes if their predominant coping strategieshave been unhelpful is in relation to it as well. Maybe that’s partof construct their resilience. Coming back to Colin’s pointof information being important, what attest is there that informationhas an antidepressive gist? I don’t know of evidencethat report alone has only one antidepressive influence. It’s just a basic thing that you needinformation you understand so you can manufacture difficult decisionsand live with the consequences.It’s just basic good attention. The difficulty for peoplediagnosed with prostate cancer is , noone with cancer expects a selection. I don’t know how many timesI’ve had somebodies told me to me, what’s this business of, I’ve got achoice, and one is, I don’t do anything? Don comes back to the GP because he’shad the bad news from the urologist. The urologist says, there’s no rush, go and think about it. You can have a radical, you can have two types of radiation or we can watch and waitfor a couple of years and view what happens to your PSA heights. It’s only 7 at the moment. You’re not going to dieif we wait for a year or so. He goes home, he’s forlorn, furious, and he’s dragged in by his partnerto see you, Caroline.She says, he needs help to make a decision. Sit down, Don, and listen to the doctor. In his situation, “its hard”. As GPs, we draw on experiencefrom previous patients or narrations we’ve heard. We have to empower the patientto make a decision using information they’re given. One thing tested in general practiceis to use problemsolving therapy. NORMAN: How does that work? You work with the patient to generate a list of the problems. In this case it might be as simple aschoosing which regiman. You work with the patientto generate as many problems associated with that as is practicable. There’s still cognitive restructuringinvolved? No , no. It’s a very structured approach. You can download structuredproblemsolving worksheets off the internet if you’re so inclined. It’s not a difficult procedure to learn. It’s just steer the patientthrough that decisionmaking process, making as many solutionsas possible, then rolling them and looking atthe pros and cons of each. It is quite an effective therapy, but probably a hard case to start with. If you want to have a goat problemsolving therapy, you might not choose a distressed manwith prostate cancer as your first subject.Try it on yourselfor on a more simple case, then if it use, try it with person like this man. If there’s more than one clinicianinvolved, we need to get our narratives together. That can cause more confusionfor the patient if we’re giving different floors. We need to do thaton behalf of the patient, otherwise it becomes confusing. A nanny in Northern Queensland expects,’ Are there anyantidepressant prescriptions contraindicatedwith prostate cancer ?’ I’d start with the antidepressantsI’m used to using. I’d help ones that don’t interferewith urinary capacity. I don’t know if there’sa strong proof cornerstone for that. I’d start with SSRIsrather than tricyclics,’ lawsuit tricyclics have urine evidences. Obvious SSRIs, the sense I get from the panel of experts is, they’re pretty muchall in the same bunch. Some have slightly different advantages. They do have sexual side effects. That’s true, but that’s going to be aproblem with all of the antidepressants.You have to make a decisionof how severe the manifestations are. Again, if someone has had thesetreatments and they’ve worked, that’s a reliable indicatorthat they’ll study again, or are at least worth trying. The same harbour in Queensland questions ,’ Should all men on hormone medicine be automatically prescribedantidepressant remedy ?’ I wouldn’t do that.I can’t see any reason why you would. If they weren’t having those specificside effects, I don’t think you would. You’d do it based on the severityof their symptoms and their preference.It’s been awhile since we hada question from Western Australia. Too a nanny.’ Is there any informationon suicide rates in patientsdiagnosed with prostate cancer ?’ There was a article publicized recently, I’ve got a feeling it was European data, which presented an increasein the relative hazard of suicide in males with advanced prostate cancer. I’ve certainly had knowledge of men with advanced prostate cancercommitting suicide. It’s somethingyou certainly never forget. I don’t have accurate data on that. And I approximate, though, the main point is it’s more about anybody who’s got depressionneeds to be screened for suicidality.NORMAN: You’ve just got to ask the question? You’ve got to ask that question. NORMAN: Do you ask the question, Peter? PETER: I certainly do. It’s not the first issue, but if I think they’ve got mildto moderate feeling, I always ask whether there’s selfharm. Given that you’re seeing menin men’s places, how do you involve the partner? NORMAN: They’ve got to be involved. Sometimes men are now in becauseof the partner in the first place. So the partner may be involvedfrom the word go. NORMAN: You precisely don’t necessarilysee them right off. It can be. That’s issues and questions we too ask how are travelling, how is your partner tour? I often go into the relationship and askhow he sees the relationship is. If the discussion wants to go onfrom there, I volunteer whether it would be of benefitseeing them both together. That’s a really positive move, peculiarly if he agrees to that. Caroline, do we know to what extenttreating the man cures the woman’s feeling? I don’t think I could answer.I principally meet womenwho are worried about their partners. I find talking to them can help themdeal with their partner’s feeling. I can give them generic policies. The risk factors Suzanne spoke aboutfor men could apply to women more. If they’ve got a history of feeling, they could be at major hazard. That’s right. Making things betterin such relationships or a family situation moves things better for everyone, but whether you are eligible to automatically assumethat treating the man will stir the woman better, it dependson the severity of his dip and how it’s impactingon their problems. If the thing that’s worrying heris that he’s going to die or be impotent forever, treatinghis dimple might not help her.You have to have a conversationwith the individuals. If you merely attend one partnerand the three men views another doctor, it’s easier if the doctoris in the same practice. I’ve had that discussion of would it be OK if told his doctoryou came to see me? So he’s aware of your concerns. There’s issues of confidentiality. But if “youre telling”, these are things we could do to help, often they’re open to that. You have to respect people’s orders. NORMAN: Was your wife chilled? Yes. One thing we have learned, and willpass on as a testimony to other parties, is that if the manis suffering depression, look at your partner as well, or your carer, why it is dragged down as well.One changes the other. Did she receive treatment? Yes, she has. She was worse off then I was. NORMAN: Certainly? Yes. NORMAN: How was it changing her? Withdrawal, attracting away from things, not wanting to go anywhere , not driving her automobile, not wanting to go shopping. It was quite a thing, to drag her out of herself. She became very much a homebody, got into her plot. While you were off on your bikein the sunup, she was in the plot, pottering around. I was embed myself inprostate cancer work. NORMAN: You were living parallel lives? Basically, yes, Norman. It wasn’t very good, it was very poor. It’s the one thing to pass on to beings. I don’t think enough attention was paidon the problem that would come of this businessof depression. It wasn’t in our case. It’s only when it was too latethat it was noticed in me because of my crankiness, then suddenly she came down too. I say it was too late. It should havebeen picked up way before. NORMAN: Suzanne? SUZANNE: I made in accordance with all of that.Carers, it is very important to especially am concerned about. There’s desegregated makes on whether carershave more distress than do cases, but there’s enough that suggeststhat in many cases they do. In our experience in running trialsat Cancer Council Queensland into psychological interventionsfor parties with cancer, we find carers are relatively difficult, comparatively, to draft into tribulations because they thinkthey don’t really tally. I’m busy looking after my partnerwho’s unwell, and I don’t have cancer, so I don’t deserve that support. They forget themselves while tryingto support the person who has cancer.When you’re looking after someonewith cancer, you have to be as concernedabout their development partners as you do about that personwho has cancer. Don and his partner Glenda come backto see you, Caroline, a year later. He’s had a progressive. He’s got erectiledysfunction. He’s had it for a year. He’s got a bit of incontinence. He’s been dragged back by Glenda, ratherthan volunteering to come and see you. She tells you he doesn’t sleep, he’s not eating well, doesn’t want to get out and about. She’s pretty distressed, more, and tells the sort of storythat Colin tells.What are you going to do here? Certainly my relapseprevention strategy from the first part of this casedidn’t work so well. NORMAN: You don’t need to beat yourself up. I’ll told me to him, I “ve told you” ifthe indications came back, to talk to me. It’s great that you’re here now. Clearly, that sounds likehe has the indications of depression, but I would completea more thorough evaluation. NORMAN: You’d go into full state. Ask all the questions. There’s a list of symptomsyou have to have to qualify for a DSM diagnosisof depression, but in general practice, we tend to think more dimensionallythan categorically. If people have got distressat a sufficient level, we start talking aboutmore proactive treatment. In his suit, I’d come back to what’s worked before. If he has evidences of recession, medicines that have helped himin the past should help again, even though circumstanceshave changed. These therapies work for the symptomseven if you’ve got another diagnosis. But you have to be aware thatmedications have side effects, which you’d revisitif he’s had them in the past.Suzanne, this notion of stepped care.You talk about the pyramid. Certainly. We have developedin Queensland a tiered sit of care that’s been widely usedacross the country. The quintessence of thisis to acknowledge the fact that, while we’re talking tonight particularlyabout extreme recession or feeling, most people will do well over timewithout deeper psychological caution. At the bottom of the pyramidis where most people are. What they need is effectivecommunication from their clinicians, access to support groupsand cancer helplines Cancer Council Australiaruns those sorts of things to know there’s a Peter around ifthere is one, to have a caring GP. That’s what most people need. You’ve got a booklet, haven’t you? We produce various. There’s a beyondblue bookletwe’ve encouraged to, a general wellness volume, a sexuality after prostate cancertreatment booklet that’s on the Andrology Australiawebsite. There are lots of resources. beyondblue have a stack of themand cancer congress have them.There’s an excellent display of resources, Cancer Helpline is a national service. If you’ve got someonewho’s got mild to moderate distress, they’re further up the pyramid.They’re a smaller number. They need care with a deeperbut narrower focus. They might needa psychoeducational program. NORMAN: What do you meanby psychoeducational? Teaching parties indepth aboutwhat a diagnosis of cancer means psychologically, and how been faced with that.Stressmanagement abilities, copingskills training, things you can do easily in a group. Moving up, you might wantto do rapport or family rehabilitation. At the top of the pyramidare your vulnerable people who might be suicidal ordemonstrating high levels of distress. They might need a therapist, a mentalhealth care team. You don’t muck around withpeople in disturb. You get them straight to serious upkeep. If you’re in a country townand referral informants are restriction, what’s your view of the selfhelp localities? St Vincent’s Hospital in Sydneynow has internetbased therapy, where they will offer a therapistonline.You’re not just doing internet CBT, a psychologist willactually talk to you. There’s MoodGYMat the Australian National University. Swinburne has something. They seem to have good randomisedcontroltrial evidence that they labor. Would you cite someone with cancerto one? I think so, if it was a reputable oneand I knew about it. It’s an emerging province, and important for Australia because we havea decentralised population. Remoteaccess therapiesare important for us to get populationbased translationof mental caution , not just for cancer but in every orbit. There is randomisedcontrol evidence forthese rehabilitations being able to deliver through the internetand on the telephone. For a GP, it’s knowing what your arsenal is. Wherever I live, I know these things are available on the internet and the phone. This age group doesn’t necessarilyhave access to the internet. That’s an issue, but it also dependsupon the level of distress. We’re doing a ordeal on this now. We’re offering two types ofremoteaccess, telephonebased therapy. Our thoughts are that people who areover 4 on the distress thermometer but not up around 8will probably do well with negligible telephone intervention, where the more distressed peoplewill need the higher level.That study hasn’t been donein cancer before. Is there evidencethat response to therapy is different when cancer underlies the depression? I’m familiar withcancer psychooncology literature, where there’s good suggestion to supporta range of cognitivebased cares, problemsolving therapy. One of the most wonderful studies was onproblemsolving therapy, where they targeted peoplewho once had anxiety and recession. It’s also about health economics. You’ve got a limited numberof resources. Let’s get our indepth resourcesand throw those at beings in trouble. A much of the others will do finewith goodstandard care and access to selfmanagement fabrics. Because you feel disempowered, don’t you, Colin? COLIN: Yes, you do. You feel very disempowered. I feel sorry for the country people. They would be even more disempoweredthan we are because they have no accessto people like yourselves. They’re locked up. For them to come in to the city, it makes them a week.Who’s going to do that? There’s a lot of men we’ve heard ofwho have had repetition of their prostate cancerand it’s metastasised. Too late. If somebody had been in contact withthem regularly, probably their own GP, maybe that would not have happened. They don’t have timeto go for a PSA test. Let’s have a lookat our next case study, a film studyon a prostate cancer support group formed some years agoby David and Pam Sandoe. It’s based atthe Sydney Adventist Hospital in the Northern Suburbs of Sydney, and proposals a peculiar substantiate base to humen and their partners with prostate cancer. MAN: The the consequences of being diagnosedwith prostate cancer varies between individuals and couples. I opted for the revolutionary prostatectomy. Once I went over the original diagnosis, yes, I was anxious, but together as a duo, we’ve been able to handle it.There are other duos not so luckyas Pam and I. They’re the peoplewe’re trying to look after. Some guys are in tunnel vision for along time after going their diagnosis. They don’t want to speak about what canhappen in their therapy alternatives. It’s usually the wifethat has this huge learning curve, and knows more about the diseasethan the partner does. We need to know if there’s a situationwhere that maiden needs additional relief. She’s probably got anxietyand depression herself, rather than merely the malewith his recent diagnosis. It’s easy to talk to peoplethat ought to have similarly diagnosed. Through the brace group, we can match people upwith whatever they’re going through.I can think of one couplewho came to us in some despair because they weren’t communicatingwith one another. He didn’t talk about it at work, and when he came homehe didn’t talk about it. Somehow, they came to our backing groupand we generated them some facts. We opened them a link with medicalprofessionals that could help them. Now they’re a great couplethat assistant telephonecounsel parties going through a similar situation. beyondblue information about anxietyand dip, the women, you can see going through it.They’ll take the fact sheets. As Pam was suggesting, they’re the ones that will workthrough things in a realistic way. Mostly, they’re the state managersof their own families, we find. We get to the men through maidens. It’s amazing how many times, and we were exactly the same when we found out the prostate? What’s that? Where is it? What’s it time? It’s not like ladies, who know they’ve gotall the different sex percentages to them.Men contemplate as long astheir penis is functioning precisely and they’re having enormou copulation, that’s all there isto the anatomy of it. They need to speak to their partner and talk to other workers, if they’re brave enough, to find out howthey can best move forward. My erectile functionand urinary function are returning pretty well, I’d say to 90% to 100 %. It’s good to be able to express yourselfin front of people. As you see today, you can talk about anything at all. I experience coming. It’s companionship. My wife has enjoyed coming alongas well. I like to spread the word. I swim every morning, and I have circulars in my pocket. If I insure a new person in the dressing room, I say, would you like to read this? There’s so many insensitive peopleabout prostate cancer. The opinion I’d givemedical professionals giving information to their patientsabout mental health is that they’ve got to be mindfulof the distres and mood of depression that beings get in when they don’t, for instance, have full sexual reclamation. They’ve got to think beyondthe diagnosis and the therapy of the disease in its crudest anatomy, thinking more about get the person backto normal of life, or as regular as possible.Now more and more, beings are being aware of anxiety and depressionand how it changes the family. David and Pam Sandoeat the San in Sydney. It’s not for everybody though, is it, Colin? What, support groups? NORMAN: Yes. Probably not. A quantity of beings prefer to haveonetoone home treatment. That happens on a few opportunities. Generally, with a supporting radical, it’s the man and the woman who come in.You get the pair of them. The subject being draggedwith his ends skidding soil. Only about. It’s jocular, but yes. NORMAN: How long does it take on averagefor the lamp to go on? What, in getting something done? Realising that, I don’t need to resistcoming. This is not for wimps. It’s something that’s good for me. Some people, it’s usually a year before they truly get involvedwith a carry group. NORMAN: Actually? Yes, as long as that. A spate don’t come straightaway. Some do. They come beforehand. NORMAN: Which is what you did? Yes. A plenty of the guyswho are keen on themselves come before any procedure is done. That’s where they gettheir road map from. Peter, what are the benefits and limitsof support groups? The benefits are enormous. I’ve talked to a few support groups. The first thing I didis see how many collaborators there is indeed. There were 20 men and 20 womenat one in Bendigo.It was a terrific social eventas well as education. But I concur , not every guywill want to turn up to that. Which is not a problem, precisely a differentway of dealing with that subject. That’s a bloke, I repute. Men are like that. They can be withdrawn. Particularly if they’re chilled, theydon’t want to go out and be in public. We have to have our opening open to giveconsults and give them time to talk. Sometimes, I think they may benefit from talking to the guy on the bar stoolnext to them. It were not able to givegreat medical information, but they need somewhere to chit-chat. That can thrive through the clinicianif we give them more experience. Then maybe they will join thesupport group, even if it takes a year. NORMAN: How do you find a buoy groupin your domain, Colin? It’s reasonably active. We’ve got something like 70 couplesregistered, and we get a swimming attendance. That’s in Sydney. But if you’rein Kalgoorlie or the Northern Territory, is there a system of support groups? The system of support groups is done from the Prostate Cancer Foundationof Australia.They have written a listof where support groups are. Any evidence, Suzanne, that they run, beyond the anecdotal? We’ve done study ourselves. There are a lot of explanatory studiesthat are crosssectional, looking at people who goto support groups, how are they doing and what are the aspectsof support groups they recognize. They’ve been very positive studies. The important thing is that there area range of services available. Different things dres different parties. NORMAN: A menu. Which might be the Cancer Helpline, the cancer counselling service, the patronize groupor one of the volunteers from the group who’s available to talk on the phoneanonymously, your GP, your men’shealth practitioner.People need to know that some thingsmight not suit, but don’t give up. If it doesn’t seem likeit’s the right shape of support for you, try something else. In Bendigo, we range men’shealth nights.We have for nine years. We get 1,500 men out in Bendigo. Bendigo’s a 100,000 population. We’ll go out into the sticksand run these darkness, cities that have 200 or 300 parties, and you’ll get 100 turn up.At those, even though it may not bespecifically on prostate cancer, we will get chaps that comeand sneak in the back. We’ll talk about things likemental health and sex state, and those guys will absorbthat report. That’s incredible. So much for blokesnot wanting to come forward. Give them the right environment, they are able to. Particularly if you put on a barbecueand a drink, they’ll turn up, and you can talk frankly to them. Thank you all very much. What areyour takeaway senses? Colin? Takeaway message for people watching is to look at getting a proper road mapof where you’re going with some of these things we’vementioned tonight included in that, of course, the largest being depression.For clinicians to ask the questionsto the patients, then to give them timeand to listen to them. I made in accordance with that. To believethat you can make a difference by helping people with psychologicalproblems as well as physical ones. NORMAN: The prove locate is there.Suzanne? Cancer is a major life stress for boththe person with cancer and the carer. Good psychosocial and psychological careis central to good care. Thank you all very much, and thank you. I hope you’ve enjoy the programon maintaining wellbeing, dip and anxietyin beings with prostate cancer. Our thanks to beyondblue, the national depression initiative, and the Prostate Cancer Foundationof Australia for becoming the program possible. Our thanks to you for making timeto attend and contribute. If you’re interested in obtainingmore information, there are a number of resourcesavailable on the Rural Health Education Foundationwebsite: To cross-file for CPD details, completeand send in your evaluation forms.I’m Norman Swan. I’ll see you next time. Captions byCaptioning& Subtitling International Funded by the Australian GovernmentDepartment of Household, Housing, Community Servicesand Indigenous Affairs.

> Now afraid of being adjudicated by others, being selfconscious, and daily social situations and avoiding meeting newpeople, these could all be signeds of social suspicion disorder, but some mightthink No. I’m just balk, I’m introverted Doctor what is the difference? when youhave patients come in and you’re and “youre telling” …> You said it! These … and peoplereally misunderstand social phobia so let me merely show. It’s not suspicion of beingsocial or anxiety of educating, it is fear of scrutiny, evaluation, arbitration, makingit chump of yourself, that’s what people fear. That’s what they bring into theroom, that’s what they bring into the situation.> Is it like what if they don’tlike me, what are they about me?> What if they don’t like me, why if…It’s what if I’mjudged, it’s what if I I imply it’s it’s nervousnes of scrutiny, and you don’t it’s it’snot paranoia but I’m walking into the room instead of just maybe looking forsomeone to talk to or noticing a friend I’m already am concerned about anxiety of beingjudged.> you slams down and you automatically …> I’m afraid. So you knowI I perhaps I appear like a shy person but I’m just the shy person is just shythat’s a temperament or a personality trait, and shyness can be grown out of aswell. We talked about shy adolescents who blossom as adults. right But that shychild wasn’t fearing scrutiny, that reticent child perhaps simply prefer to read ratherthan be outgoing or the rowdy one in a group.> Right. Where someone withsocial feeling really is just they’re panic-stricken inside.> Right. Terrified.Terrified and you don’t know what it is.> So how do you work through something likean in social feeling because as we need to live in the world, we need to go to work .> Right. So that’s where cognitive behavioral therapy jobs highly is a good one, because with your the social socially phobic person and you tell me I walkinto a apartment and I mull I look nice, and I suppose I’m dressed well, and whateverand the first expectations I have, are what are they what are they thinking about mehow are they judging me, what if I say a stupid thing, what if the wrong wordsfell out of my mouth So I asked you, well have you had any evidence but that’sever happened ..
A cure is a substance or procedure that ends a medical condition, such as a medication, a surgical operation, a change in lifestyle or even a philosophical mindset that helps end a person’s sufferings; or the state of being healed or cured.
A disease is said to be incurable if there is always a chance of the patient relapsing, no matter how long the patient has been in remission. An incurable disease may or may not be a terminal illness; conversely, a curable illness can still result in the patient’s death.
The proportion of people with a disease that is cured by a given treatment, called the cure fraction or cure rate, is determined by comparing disease-free survival of treated people against a matched control group that never had the disease. Another way of determining the cure fraction and/or “cure time” is by measuring when the hazard rate in a diseased group of individuals returns to the hazard rate measured in the general population. Inherent in the idea of a cure is the permanent end to the specific instance of the disease. When a person has a common cold and then recovers from it, the person is said to be cured, even though the person might someday catch another cold. Conversely, a person that has successfully managed a disease, such as diabetes mellitus, so that it produces no undesirable symptoms for the moment, but without actually permanently ending it, is not cured.
Related concepts, whose meaning can differ, include response, remission, and recovery.
Check More at http://CBproAds.com/sf.asp?id=4123832
Panic is a sudden sensation of fear, which is so strong as to dominate or prevent reason and logical thinking, replacing it with overwhelming feelings of anxiety and frantic agitation consistent with an animalistic fight-or-flight reaction. Panic may occur singularly in individuals or manifest suddenly in large groups as mass panic (closely related to herd behavior).
Check More at http://PIF43.com/splashpage2.php?ref=ralphleaman