Category: Anxiety
2-Minute Neuroscience: HPA Axis
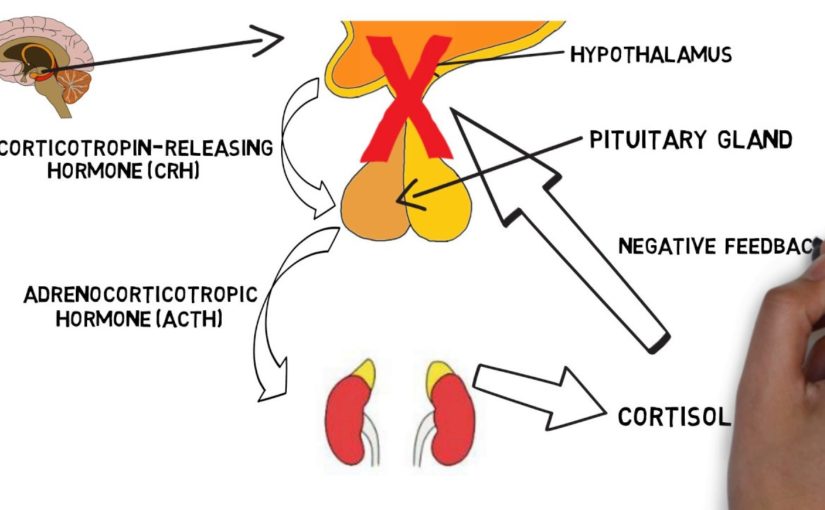
Welcome to Neuroscience for two minutes, where I excuse neuroscience topics in two minutes or Less In this batch, I will explain the HPA axis Both the hypothalamus the pituitary gland the adrenal gland, is known for its axis in its interaction with stress. The HPA axis includes a group of hormonesecreting glands from the nervous and endocrine organizations Under the hypothalamus, pituitary gland and adrenal glands The hypothalamus is the small neural endocrine arrangement set above the ability stanch Authorities the secretion of hormones from the pituitary gland, a hormonal gland Lies merely below the mulch The pituitary can secrete hormones in the bloodstream to reach a variety of purposes In the case of vehicles of the HPA axis, hormones liberated from the pituitary gland are transmitted To the kidneys and alter hormone secretion from the endocrine glands called the adrenal glands Which is located above the kidneys The primary capacity of the HPA axis is to regulate the stress response When we suffer from a traumatic thing, the hypothalamus liberates a hormone called the freeing hormone Corticotropin or( CRH) CRH refers to the pituitary gland to exude a hormone called adrenocorticotropic hormone Or ACTH in the bloodstream ACTH hastens to the adrenal glands where it expects the secrete of a hormone called Cortisol from the adrenal cortex, or outer blanket, from the adrenal glands The secrete of cortisol campaigns a number of changes that help the body cope with stress For lesson: Assists build up energy like glucose, so the body has enough vigor to cope Long press When cortisol degrees rise in the blood This is felt by receptors in the brain regions such as the hypothalamus and the hippocampus, which stops the stress response Through what is known as the mechanism of negative actions Do the rendition: Shwan Hamid Twitter:@ shwanBBBBBhamid

As found on YouTube
Antipsychotics: Classification and Side Effects – Psychiatry | Lecturio
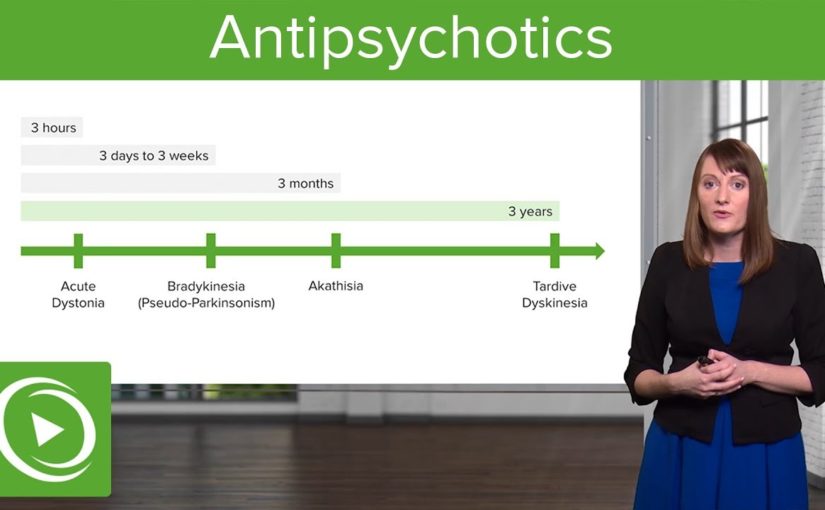
[ Music] antipsychotic therapy and pharmacology is an essential topic let’s go over the highlights here so antipsychotics are drugs also known as neuroleptics and they are categorized in terms of conventional and atypical they act by obstruct dopamine receptors and thereby reduce psychotic symptoms these are used to treat psychotic illness and too psychosis that starts along with other ailments so throughout the lecture serial you’ve learned that psychosis can actually appear as a evidence of severe depression it can also come up during times of dementia so there are a lot of uses for antipsychotics and they can occur in other patients who don’t merely have a primary psyche insane illnes as well so let’s go through the two types usual and atypical well a few examples of ordinary neuroleptics include chlorpromazine thyroid is een haloperidol a typical examples are things like risperidone and ziprasidone so the normal neuroleptics these are d2 dopamine antagonists they have a quite high authority now a normal neuroleptics do annoy dopamine however their lower authority for that and we are really too will target serotonin and histamine receptors as well the typical neuroleptics tend to be really good at analyse positive evidences but the atypicals are actually better at considering the negative evidences which we think of as the merits of the psychotic manifestations ordinary neuroleptics because of their dopamine siege they can really justification a great deal of extrapyramidal side effects that doesn’t happen just as much with the atypical neuroleptics nonetheless these are more likely to cause side effects like sedation and also weight gain or metabolic questions when it comes to the conventional neuroleptics there are again two subtypes there’s the high capacity normal neuroleptics and too low-toned capacity conventional neuroleptics so we’ll talk a little more about those last-minute and for the atypical Nora as I said before these tend to not only block dopamine but they likewise have a strong affinity for serotonin alpha receptors histamine receptors as well in serotonin so the antipsychotics basically again these target dopaminergic neurons that’s really the key and there are a few different dopamine pathways that you should be familiar with the nigrostriatal the Me’s a limbic and the tubero infundibular now neuroleptics are highly overweight soluble and therefore there are a lot of options for returning these intramuscularly or through an dose we’re gonna review that later but as a teaser it’s important to know that when it comes to taking an antipsychotic medication sometimes patients are very fomented in the hospital setting and it’s really nice to have the option to do an insertion of remedy likewise some people don’t like taking a pill every day and the longacting injectable antipsychotics actually allows users by monthly or monthly dosing which can be a nice option for cases so there are a lot of different squanders for antipsychotic prescriptions some are of course the primary psychotic diseases too mood conditions like mania and depression and Tourette’s disorder they can also be helpful there so let’s talk a little more about the conventional antipsychotics and let’s start with the low-pitched effectivenes wands so these have a little bit of a lower affinity for the dopamine receptor and patterns include cor promazine and thioridazine now there’s a higher incidence of anticholinergic influences with these remedies and a lower incidence of the extrapyramidal side effects that can be very upsetting to patients also a little of a lower incidence of neuroleptic malevolent syndrome which can be a deadly side effect of antipsychotic prescription the high capacity conventional antipsychotics have a very high affinity for dopamine siege and these include haloperidol flu phenazine and some other examples listed here there’s a very high incidence of EPS or extrapyramidal indications with these medications and also neuroleptic malignant illnes lower incidence of anticholinergic and antihistamine troubles so what are extrapyramidal side effects you might be wondering so it’s very important to know for your cards so extrapyramidal side effects come from dopamine blockade often through that nigrostriatal pathway and a very early ratifies of this can be acute dystonia now this might attest in your case as something like an oculogyric crisis where their seeings kind of roll up in their honcho it can also be seen as torticollis or next stiffness and acute dystonia can be very distressing to a patient and it can occur immediately or within hours next another eps evidences is brady kinesia or parkinsonian indications so this can look like masked facies where person doesn’t have a lot of expression it can also look like cogwheel rigidity which you might test for when you’re doing your physical exam on a patient some patients have this brady kinesia or hindered changes and they also can have a gate where they do something which is called turning on block meaning that they will make a sudden stop and then turn their entire body so it’s not very easy for them to shift and maneuver as it is for the rest of us they may also get a tremor which can be a cardinal peculiarity of a parkinsonian side effects from this prescription another difficulty that can occur within months of starting an antipsychotic medication is akathisia this is highly distressing to patients so what akathisia is is it’s an internal feel of restlessness it will often evident as a patient pacing perhap sounding their foot or their hand on their leg they’ll often describe to their doctor that they just feel like they want to crawl out of their surface so that’s a sign of a Cathie’s which again is very distressing and then a really important side effect of antipsychotics to be informed about is tardive dyskinesia now it can take times and even decades for a patient to develop tardive dyskinesia a little pearl for your quiz is that elderly Caucasian ladies her hat highest risk for developing tardive dyskinesia when they’re is dealing with an antipsychotic so what this actually looks like is abnormal shifts for example of somebody’s face you may see someone fastening their tongue out frequently or smacking their cheeks together this can also occur less frequently in boundaries or truncal areas and the really unfortunate thing about tardive dyskinesia is that in most cases it’s actually not reversible so it can be very permanent and a disfiguring side effects both traditional and atypical neuroleptics have similar efficacies in terms of treating positive indications of psychosis now you might remember the positive indications of psychosis or things like hallucinations hallucinations bizarre actions however when it comes to treating the negative symptoms of psychosis things like having a flat influence little motive good vigour speech alodia that’s better treated with one of the newer antipsychotics or atypical antipsychotics so the traditional antipsychotic side effects to review them are anti dopaminergic anti ham which we’ll go over that in more detail in a minute of course tardive dyskinesia and dystonia or in other words the EPS symptoms including brady kinesia and akathisia neuroleptic malignant illnes which we’ll talk about in more details too a serious side effect so in terms of tardive dyskinesia we spoke it before but another little pearl to know this is riding movements of the mouth and tongue when your patient is described as having that judge tardive dyskinesia the anti dopaminergic sideeffects is certainly the extrapyramidal symptoms too hyperprolactinemia and this is due to interference of dopamine in the tubero infundibular pathway so cases have been able to end up with so much dopamine blockade that they get a surge in prolactin and this can manifest is actually lactation from the breast and it can occur in women but also in men and then neuroleptic malevolent disorder is another extremely noteworthy sideeffect to look out for so I mention anti ham side effects before well let’s talk about that aims so that H is antihistamine where patients can become very sedated the a is anti alpha adrenergic side effects this can look like worth a static hypotension cardiac arrhythmias and sex dysfunction the anti muscarinic side effects include baked lip tachycardia urinary retention misty vision and constipation all things that are of course undesirable to your case they may also get force income promoted liver enzymes they may have eye difficulties or off the malla reasoning problems dermatological problems and seizures and because tardive dyskinesia is so incredibly important in a potentially irreversible and deforming side effects we’re mentioning it a good deal here it’s really important to be informed about for your quiz and it’s really important to note that it can lead to that permanent disfiguration if you have a patient showing signs of tardive dyskinesia you really want to consider lowering their dose of antipsychotic giving them a drug holiday from their antipsychotic or switching them to another worker preferably an atypical antipsychotic[ Music]

As found on YouTube

Grounding Technique for Anxiety #10: Square Breathing
this next a instruct act is calledsquare breathing and square breathing can be useful for a couple of reasonsone because our gulp is connected to both the one of the purposes of our nervous system thatwe can control and the one of the purposes of our nervous system that is automatic so ithelps us access that appeasing part of our brain kind of in through the back doorthe other thing about square breathing is you practice it with motley lengthsof wheezes then you can practice frame yourself into a slightlyanxietyprovoking situation which is being out of breath but you’re doing itintentionally in such a way that something that are usually be anxietyprovoking or embarrassing becomes something that you can administer withwillingness so you are basically converting something that might havebeen traumatic into something that is very comfortable and that drills yourbrain to believe that you have the ability to convert something that’sstressful into something that’s beneficial for you so let me justexplain square breathing really quickly so with square breathing youimagine yourself breathing a long a square so you imagine yourself startingat the top right corner of the square and you imagine yourself breathing in forfour seconds and then you imagine yourself holding that breath for fourseconds and then you imagine yourself breathing out so exhaling for fourseconds and then holding that air out for four seconds and you’re back to thetop of the square and you repeat that four times so breathe in two three fourso you’re breathing in that whole time supporting it for four seconds breathingout for four seconds you’re exhaling for four seconds and then you’re stayingwithout wheeze for four more seconds so just like that when you breath you wantto have all the breath out that you are eligible to have out to want to be completely out ofbreath when you’re done with your breath you want to be completely full of breathand the other two are the process of coming in and out now you can lengthenthe amount of time that you’re doing these breaths and exhales and propping soyou can lengthen it out to eight seconds or 10 seconds or 16 seconds but when youlengthen the amount of time that you’re out of breath you’re gonna compel yourbrain to panic for a little bit and that’s where you can kind of challengeyourself to increase your convenience with being out of breath so actually there’stwo ways to do this activity the first road is to just stay at for secondsbreathe in for 4 seconds holds in store for 4 seconds breathe out for 4 seconds holdfor 4 seconds and that’s just gonna be various kinds of naturally mollifying because it’screating a rhythm and the other way you can do this is to challenge yourself tolengthen the amount of time you’re holding that breath and that’s gonna bea little bit more of a mental challenge that creates more resilience so as youdo this activity just watch yourself and pay attention to the sensations that comeup so paying attention to your gulp is going to help you stay centered andgrounded while many ardours go through you I hope this video washelpful thanks for watching and take care hi everyone I’m elicited to announce thatmy udemy course change your intelligence is now live so this is a two hour intensivecourse that goes into the ways that you can change your intelligence chemistry withoutmedication so these are very practical abilities that have been shown throughresearch to improve mental health and combat hollow nervousnes and othermental illnesses in this course I teach the practical application ofneuroplasticity which is the developing realm of science showing that our brainsare adaptable and changing throughout our part lives that our brains canactually reform their structure function and chemistry by how we envision and how weact and such courses coaches ten simple directions that you can improve your mental healthby pleasures that take only a duo minutes every day so I formed thiscourse because this is fundamental information that I think everyone shouldhave access to so satisfy take a look at it the link is in the description it’son udemy.com and I’m including a coupon code if you’d like to take the coursefor free time route me a private meaning and I’ll give you a code so check it outthanks and take care

As found on YouTube
Rewiring the Anxious Brain – Neuroplasticity and the Anxiety Cycle(Anxiety Skills #21)
So here is the amazing thing about your ability, it’s made to rewire itself all the time. This is called neuroplasticity. Scientists believed that after childhoodour ability was pretty much locked in place, but now that we have better likeness technology, we are able to literally see how the brain deepens depending on how we use it. So, in this video I’m going to talk aboutone very simple thing you can do to rewire your brain to be less watchful, and it is simple, but it’s not easy.So I’m also going to share three steps youcan take to make it happen, and share ten extra skill you can develop on your own, orwith a therapist, to build up your ability to take control of your feeling. And if you would like to learn more in depthinformation about how analyse your nervousnes, I’ve got a course on Udemy that I am workingon called Rewiring the expectant brain, so you are able to check out that tie-in in the description. So, let’s start off with one example of neuroplasticity. In London the taxi moves have this superdifficult exam where they have to prepare by learn all of the streets and eventsand places in this huge city.Researchers took portraits of their ability beforethey started studying, and after this two year process and they only literally ableto see the brand-new neural connects, the wire that changed in the intelligence. And there’s good evidence that changing howyou think, like going to therapy, can actually change the structure of your psyche and thetypes of chemicals that it’s running out. Our brain has an amazing ability to rewireitself to learn, flourish, and mend. So, let’s talk about how to do that with tension. If we want to change how our brain processesanxiety, we need to understand three principles of anxiety. Number 1, we need to understand what is anxiety. Now, this may sound dumb, because you alreadyknow what anxiety feels like, but what you need to do is understand your perspectiveon anxiety. You need to let go of the relevant recommendations that anxietyis bad. Anxiety is not inherently bad. Anxiety is disagreeable, some times anxietyis illness, sometimes nervousnes does in accordance with the arrangements, but we all experience anxiety becauseit is supposed to serve a really important function.To motivate us to avoid real danger. We’re supposed to feel expectant when standingon a cliff hem, it helps us be safe. We’re supposed to feel desirous when we knowwe have an important test coming up because that should cause us to study. Anxiety tells us that something is importantto us. Anxiety and hullabaloo are basically the samechemical reaction in your organization with adrenaline triggering that affectionate activating andprepping you for action. When we look at anxiety as unpleasant, but acceptable and a regular part of life, unexpectedly we develop new tools to work withit, and that includes working with the other type of anxiety.So, the second thing we need to understandis we need to understand ailment distres. And this is when anxiety seems to take overyour life. This is anxiety that establishes it hard to go towork, to clas, or to enjoy life at all. And the harder you try to make it go away, the stronger and stronger it gets. Now, contrary to popular belief, that anxietyis agitation when it is more severe, anxiety is actually ailment when one of two thingshappen. When, number one, when you feel endanger whenyou are actually safe, and I made a video on this, it’s called perceived vs. actualsafety. For illustration I is cooperating with a patron who wasafraid of radiators. She would feel anxious and sweaty around themand she couldn’t represent herself go into a chamber with a radiator in it , now radiators are not actuallydangerous, but she was having a real, physiological response to something that was actually safe. So tension can be illness when you havea danger response in your form, but you are actually safe.The second mode feeling is likely to be disease is when your tension interferes with your ability to function. This is essentially what determines if youmeet the criteria for an anxiety disorder diagnosis. When your nervousnes, or your attempts to avoid anxiety stop you from effectively facing life. When this happens you start avoiding school, or calling in sick to work. You stop leaving the house, or spend timewith friends, pretty soon your feeling is taking over your life and stopping you fromdoing the things you desire. So causes talk about what causes anxiety to coiling out of control. This is called the anxiety cycle. Every day throughout our daytime “were having” events and we understand these experiences as either being safe or dangerous.So make say for example you determine a dog. Now, each person performs an experiencedifferently, for some people this would be extincting and fun, but for some reason youthink, that dog is going to bite me! This leads to feelings of horror, anxiety, maybeeven panic. These are unpleasant feelings and you may even make them as a clue that your thoughts are true. So, you escape, you run away, you get outtathere.And, Nothing bad happens. So your brain liberates this flood of easing, Whew! That was close! The only way I subsisted was because I ranaway. I could have died! And your intelligence judges I better do that again, I’m going to make make human avoid that situation by increasing their anxiety about it. And, vola! your nervousnes goes up. Every single time that we bypass a threat andsurvive, our mentality conceives, Let’s do that again. So it lays down neural pathways, this wiringthat reinforces that behavior. And the whole function of affections is to motivateus to action, but that’s a whole other video. So our mentality, because we have persuasion itthat the dog was a threat, it shall take such action into it’s own hands and it increases you anxietylevels around dogs.Every term we feel suspicion, and then avoidthe situation, our nervousnes height will go up a notch. So this is principle number three, avoidancefeeds illness suspicion. It literally originates devastating feeling. Now, there are lots of ways to avoid. There’s running away, and physically shunning, but there’s also feelings escape, so if you have social anxiety, you might still goto the party, but only if you get drunk ahead of time, or you might be in a relationship, but scared of getting hurt, so you don’t allow yourself to let the other person into yourheart.You stand emotionally remote, or you protectyour self by not dedicating. social media, rage, denounced, distraction, andeven coping sciences, can be avoidant. Regardless of the type of avoidance, it increasesyour nervousnes and, all the more serious, it reduces down your world. So with the dog example, you might start avoiding situations where a puppy might be present, by not going to friend’s homes, or bouncing thepark. And your world contracts, you miss out on goodrelationships, or you stop going to parties.And your world gets more and more restricted. Avoidance can perform your world tiny and scaryand happy. But each time you get anxious and eschewed something, and live, your psyche multiplies your nervousnes in that area. Now, looking at this cycles/second, “were having” two placeswhere we can intervene. Where we can stop that anxiety from spiralingout of control. The first place is with our actions.When we feel suspicion, but we are actuallysafe, if we stick with it, if we stay there, we experience our ardours and sensationswith out running away, and again, if you do this, and you don’t die, then your psyche learnswhew! what a comfort! I guess that not all pups are dangerous, let’sdo that again! And it sends out a surge of succour. This leads to a gradual decrease in anxietyover time, and a gradual increase in your feelings muscles, your ability to feel sentiments and impressions that are unpleasant, with out needing to escape them all the time. So you to be all right at feeling. As you do this your brain literally lays downnew neuro pathways saying not all bird-dogs are dangerous, I don’t need to be anxious arounddogs. And it literally changes your brain chemistry, liberating less cortisol and adrenaline and other stress hormones.This is the most straight forward way torewire your psyche to have little nervousnes. But, I get it, this is super hard-boiled. If “its been” easy, you would have already doneit. So I’m going to break it down into three bigsteps for you. Now on a line-up greenback, the second place in thiscycle to intervene is with your thoughts. Changing how you think about the dog. And this can be a potent and efficient treatmenttoo, but it can also get really complicated. And it is more efficient before your expectant, ratherthan during. Now I can talk about some of the ways youcan change your thinking in other videos, but in this video we’re going to talk abouthe most straight forward way to rewire your expectant intelligence and that’s through your wars. So, how to get it on. There are three steps. So step one, make an exposure hierarchy, I’ve made and entire video about this, but mostly you take one thing that scares you and youbreak it down into teeny minuscule paces, and you start by courageously facing the easiest onefirst.Now this is the part that most people miss. They jump in too fast and then they panicor the flee and they never make love again, and then that fright is reinforced. So make and exposure hierarchy and write downas countless teeny little steps as you can think of. Step two, deepen your rules. Now, spirit doesn’t mean the absence of fear, but preferring that something is more important that by-passing panic. In acceptance and commitment therapy, thisis called willingness. Allowing yourself to do something even thoughit makes you awkward. If you make a rule for your ego like, I’mgoing to do this until I get too watchful, then you brain will be like cool, let’s dothat, then I can escape. So it will constitute you really anxious, and whenwe say I’m going to do this thing unless in reaches me desirous, then we are just invitinganxiety to make all of our decisions for us. So when it comes to exposure, you choose aneasier activity to start with and then you stay with it and watch yourself for a certainamount of time, or until your nervousnes increases by half during the exposure.Now, while you’re facing your nervousnes andpracticing your willingness, footing works, and selfregulation activities, this bodyupapproach to weakening feeling can be useful. But the most important part is that you sitwith your feeling for a little while until it declines, or at least for a certain setamount of duration. Now, step three. Do it. Face it. Go get anxious and see if you live. A little spoiler alerting here, you will. So with the dog example, start be repeatedlyimagining yourself interacting with a pup and you rule every day for ten minutesuntil that activity no longer originates you very anxious.And then you might want to work with a friendwho has a dog to set up the nest paces. So you might check a hound through a window andjust stay there and you sit with it and you breath with it and you allow your self torelax and you do this every day for ten minutes until your nervousnes reduces. And then you pattern being in the same roomwith a insignificant puppy on a leash, and the perhaps touching a tiny dog on a leash and then pettinga tiny dog on a leash and eventually you are moving up to a bigger dog and the off a leashthen eventually you get your self to the point where you can go to a pup common, sit down, and stay there for thirty minutes. It’s ok it you feel uneasy. It’s ok if you feel uncomfortable or you sweat, or you shake, or whatever, but you time stick with it. And pretty soon your mentality learns It’s cool, most pups are safe, your ok. And your feeling will decrease. Now again, you can do some physiological groundingactivities while in the midst of your suspicion, but don’t use those as another way to justavoid anxiety.Use those as a highway to practise willingness. This willingness to feel what you are feelingand professed it as being regular, natural and ok. So there’s the simple solution to anxiety. face your suspicions and they will decrease. This may seem too simple, or too absurd, too big of a bounce, so therapist have organized a assortment of ways to break that leap down intoa knot of tiny paces, a bunch of talents that you are eligible to learn to make it easier. If you want to go more in depth into thatlet’s do that. Let’s talk about the more detailed processof how we do this. The specific skills that help us move fromanxiety avoidance to ability over our nervousnes. Because I am trying to cram so much informationinto this topic, I’ve decided to split this video up in to two parts. So check out part two for the ten knowledge youcan develop to help you face your nervousness. Gradual exposure therapy, which is what Ijust described, is a researched backed approached demonstrate to help reduce anxiety and plow anxietydisorders.It does this because it literally changesthe mentality. Rewiring the neuro pathways and changing therelease of substances in the brain. So make sure to check out my part two withthose ten talents to assist you face your frights and if you’d like to learn more in depth informationabout how to treat you anxiety, I’ve got a course on Udemy that I am working on it’scall Rewiring the Anxious Brain, so you can also check out that associate in the description. Now, please share this video, you never know who might benefit from it, thank you for having watching and take care ..

As found on YouTube

Children’s Anxiety: 3 Ways to Help Your Anxious Child
Childhood is supposed to be a time for merriment , not annoy. But an alarming number of our kidsare feeling desirous. In actuality, the Young Minds Matter survey conducted by investigates at the Telethon Kids Institute found one in 14 Aussie babies has an anxiety disorder. There are lots of common causes of anxiety in teenagers and lots of different reasons why children will worry and that they are able to likewise differ by their age. So, for example, dissociation suspicion is a regular developmental theatre that happens for all children at around six months of age and that’s totally normal. For little kids, common fears are things like roaring noises, the dark, being separated from mum and dad strangers, swine like pups, ogres, that kind of thing.And then as girls get older their perturbs change. They might start upsetting more aboutfitting in with friends. Being admitted at school and amongst their peers. Performing at school, performing at boasts, or music, or whatever it is they do in their spare time. But how do I know when to worry about my child’s level of dwell? When it’s getting in the way ofnormal everyday pleasures, so for example if I get a bee sting on my hands I might feel a little hesitant the next time I investigate a bee and that’s a completely normalcommon reaction that we’d all have. But if my dwells get to the extent where, say, I don’t want to go the park to play with my friends anymore becausethere might be a bee there, or I’m too fearful to leave the housein case there’s a bee outside that’s when we start to think okay I might need to secure some additional help here. And Jessica has three main tips-off to assist you manage your child’s anxiety.ONE: Talk about it Talking about what anxiety is, what that might be like for your child and working out what their provokes are so it might be working out where in their body they feel nervousnes. A absces tummy today or a race nerve. Or if you notice your child’s looking watchful talking about what thinkings they might be having, so, what’s constitute you conceal today and then talking that through. The point is not to get rid of anxiety, that’s quixotic, all children will be anxious. It’s to help your child understand that they can tolerate and cope the distress associated with anxiety, so that nervousnes itself doesn’t become a shocking thing. TWO: Model healthful behaviour So if you’re feeling emphasized say, Look mum’s feeling a bit stressed at the moment and talk about how you’re getting through that, so I’m going to take a few big-hearted penetrating wheezes I’m going to think about what the problem is and what possible solutions there might be, and then I’m going to feel better immediately the concern passes. THREE: Validate their feelings So for example, your child might be feeling reallyworried about a math test.You might say Course you’re you’re feeling obsessed, math assessments are a bit scary aren’t they? and then you help them to confront that fright and say okay, you can take a few deep breathers, you can tense and relax your muscles, you can practice some maths at homeso you feel prepared for tomorrow and then you help them to confront their dread so that they know that they can deal with this anxiety and that it’s going to be okay. If you still have concerns … If a parent is really worried about their child’s levels of anxiety and they think they are getting to a pointwhere they’re getting in the way of their child living outtheir everyday life, there are definitely lots of places to seek help.First port of call could be their GP, and they can help you get in touch with community services or private works like clinical psychologists who can help your child talk through their dwells with things like cognitive behavior therapy ..

As found on YouTube

Anxiety and Sensory Processing Disorder – Which Comes First?
So today we’re talking about sensoryprocessing ill and suspicion and which comes first.Is it sometimes that we get anxious and therefore we become sensory reactive andsuper sensitive or under energized or is it that our sensory causes theproblem and this is a really good question and it’s a really important oneto address well so we’re really just going to introduce some of the conceptsjust now and generating some things into the room that we need to think aboutwe’re not going to solve all the problems that the issue fetches upbecause that would take days.So let’s give it a go from anoccupational care position when we think about sensory processing disorderand anxiety we’re really starting to wonder if the distress that our client is carrying is really secondary to the sensory processing disorder thechallenges that that generates and so that’s really where I’m going to speakto today and we will bring in a psychologistlater to talk about when feeling is the primary part of the picture and more ofthe root cause of what’s going on. So if we think about the sensory systems andreally try and unpack them and go deep with what it might mean to have adysfunction in one or many of them then we can start to understand that it wouldnaturally be a cause of nervousnes because fluctuation needs to be organized and underour assure to feel safe our sensory structures have a awfully primitive functionof impeding us alive as well as helping us to move, move beautifully, move withfinesse, navigate gaps and become social creatures.The firstly patch though is this safety keeping us aliveOur sense of balance, our vestibular sense that spirit level ofliquid in the inner ear and quartzs that tells us if we’re upright againstgravity or where we are that method, its first part is to keep us aliveand if we get turned upside down real quickit’s gonna make all the alarms go off and it’s going to be telling us that weneed to change something pretty quick so we go into a regime of flight or into astate of push or even more serious into a freeze district when this system sendsall the alarms off.Also when the system isn’t getting enough informationit starts to wonder if I’m safe and alarm systems, alarm bells start to ring.So for example if you’ve ever been in an elevator and there’s that time beforeyou can really tell if you’re moving yet or not, there’s that instant andpeople start to look at each other like are we okay? what’s about to happen here? because we’re not had enough data sufficient information from our vestibularsystem to really assess if we’re safe, if the situation is okay which course we’removing. And again that sense of frighten that you get when you’re on a publictransport, maybe a bus and the bus next to you which one’s moving is it me orthe bus next to me? My visual arrangement and my vestibular arrangement are in conflict andI can’t tell what’s going on, I go into alarm.So these are just examplestrying to help us empathize with individuals who struggle with theirvestibular information on a daytoday basis and that state of deepened fright, arousal that they get into or that they exist in for most of the day, which wouldlook like an anxiety disorder but it’s not it’s not clinical nervousnes in thosesituations, it’s anxiety that’s caused by a lack of integration of the vestibular arrangement with perhaps other organisations contesting report , not enoughinformation and being too quickly and too often in a state of oppose or flight orfreeze.The same falls for our position sense our proprioceptors which arepredominantly in our joints and when we get compression or when we get tractionon our seams we know where we are in space. I often would fall asleep on myarm and go to that level past pins and needles when my limb is just like is iteven there ?! and that if you’ve ever known that is really alarming, thealarm systems go off and your mas starts to say this is not okay, I’ve losta whole limb here and you know what’s happened is that there’s that blood flowhas been a problem, the proprioceptors aren’t serving very well.Your senseof proprioception maintains you fastened and grinded in your own body and when thatsystem is inaccurate, it’s inconsistent, it’s not giving you greatinformation then your arousal goes up and you start to have alarm bells goingoff in your lower mentality saying I’m not safe, I need to be wary, I need to orientto everything that’s going on around me and that inspects again that caution, thatanxiety.But it’s got a sensory root in these cases, but we don’t call theseanxiety agitations, we’re visit that a response to what’s going on with thesensory systems and we could go on with speciman after speciman. A reallyimportant one to think about is the child who really has trouble withmultiple sensory organisations at once and the most challenging environment for thatchild generally speaking is institution because the school environment isloud, it has buzzers, it has visual jumble, there are things hanging from theceiling, there are Mobile’s, there are still posters, there’s Halloween presentations, there’s resembles in the cafeteria, children are entirely unpredictable and they slap you andthey push you and your nervous system is constantly vigilantly trying to keep youalive and you looks just like a uneasy child an vigorous child a child withbehaviors but it comes back down to sensory processing. So this is wherewe start to say with some of our children is the sensory or is thisanxiety? When this child’s at clas they cannot coping, their patience for stressis minimal because they’re using all their resources just to get through theday, or are they so stressed that they’re reactive and we need to figure out whichone comes first.And some of these children where the multisensory piece isthe problematic piece so what we do with those minors is we increase as much stressas possible, we cater to their sensory systems, we nourish their sensory plans, we settled them in the claim regiman, we look at the other accentuates in their life arethey getting enough sleep? Are they imbibing enough water? Are they eatingenough food? How are their relationships? How is their timetable? How are theygetting to school? What’s their socioeconomic status? All of thesestresses we look what i found, we nourish the sensory systems and then we wait and wewatch and we start to unpack.And if this child is able to adapt better when wenourish their sensory systems and adapt the environment, then we know thatfundamentally what’s going on here is not anxiety but that the sensorystresses are so great that they’re causing an anxiety response. But if afteradapting and treating for sensory the suspicion is still particularly prevailing then werefer we find a really good mental health provider who are familiar with sensory but we refer to them and we get them involved and we start unpacking the restof the picture and what’s going on and that’s really important. So that’s been alittle introduction to sensory processing disorder and nervousnes and theinteractions between the two. It’s sensory awareness month. I’m VirginiaSpielmann the associate chairman of STAR Institute now and weare trying to raise awareness, educate and research more into sensoryprocessing ailments so there will be a link that we’d love you to click on toshow your subsistence. Please share, note and give us know what you want todiscuss ..
 As found on YouTube
New Explaindio 4 is revolutionary technology which creates fascinating videos by combining 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video. This is why I am extremely excited to be able to tell you that now there is Explaindio 4, which is an easy to use video content creation software that allows you to combine 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video.
As found on YouTube
New Explaindio 4 is revolutionary technology which creates fascinating videos by combining 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video. This is why I am extremely excited to be able to tell you that now there is Explaindio 4, which is an easy to use video content creation software that allows you to combine 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video.
As found on YouTube
New Explaindio 4 is revolutionary technology which creates fascinating videos by combining 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video. This is why I am extremely excited to be able to tell you that now there is Explaindio 4, which is an easy to use video content creation software that allows you to combine 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video. 
Meditation for panic attacks: does mindfulness work? (The Latest Research)
Sarah queries How can I stop my panicattacks naturally? Im interested in mindfulness meditation and Im wondering, does it work for panic attacks? Hi, Im Michael Norman and welcome to PanicFree TV Q& A. This is where as research scientists and anxiety professional, I answer your most pressingquestions about how to quickly stop your panic attacks for good so that you can enjoya normal, panicfree life again. Okay, so there are two questions now: One is about how to stop panic attacks naturally. The other is about mindfulness meditation, exclusively. Gives talk about mindfulness first. Now, the research clearly shows that mindfulnesscan help with panic attacks, but its not for everyone. I’ll interpret more in precisely amoment but firstly let me take 30 seconds and quickly explain what mindfulness is, foranyone who doesnt know. One of my current definitions of mindfulnessis that its purposely bringing your full attention to the present moment, really observingand accepting whatever is happening in your current experience, without approximate it atall.Now, this is just one definition, and definitionsare always merely Aims to describe reality. If you was just going to a eatery and you merely readthe menu that would never supplant actually smacking the nutrient, and so the only true wayto know what mindfulness is like for you, was an attempt it. This can be done formally with a mediationpractice whatever it is you dedicate blocks of time to practicing being fully present, aware andaccepting of some aspect of your current experience, like your breathing. It can alsobe done informally throughout the day, simply by being PRESENT to your senses, to whateveryou happen to be doing. So how does mindfulness relate to stoppinga panic attack? Well if you’ve already watched my freePanic Free TV foundation serials then you already know thatone of the main thingsthat oils a panic attack is trying to fight it Mindfulness offers us one antidote thatof being present to, and learning toACCEPT rather than fight, whatever desirous thoughtsor body sensations that you might be experiencing.While it doesn’t immediately stop a panicattack, if you can accept and precisely be present with a panic attack, that takes away the fuelthat restrains that panic attack proceeding. As mindfulness explorer Jon KabatZinn introduces it the mindfulnessattitude is You CANT stop the brandishes, but you CAN learn to channel-surf. Now, apparently perfectly abiding a panic attackis FAR, FAR easier said than done … which is why it makes so much practice. This is reflected in the two mindfulnessbasedprograms that have been show scientifically to help with panic attacks. Theyre both 8 week planneds they both involveup to 30 hours of group instruction plus this relates to 45 minutes to an hour of meditationpractice, each day by yourself. Now, if youre thinking that this is a hugeinvestment of day, then I definitely concur. If you JUST want to end your panic attacksthen, for me, its obviously not worth it. I demonstrated in you far faster, far more reliableand far more effective ways of turn panicfree. But if youre already interested in meditation, and if youre previously considering starting your own daily rehearse then definitelydo it because there is a huge amount of research showing that mindfulness can help reduce stress, dwell, recession, even back pain, and it can increase your general sense of wellbeing.And when it comes to panic even though we need a lot more research it seems tohelp about 75% of parties over such courses of a year IF theyre willing to invest thetime into a daily mindfulness practice.Now onto the second question: whats thebest approaching to stop panic attacks naturally? Well, this is exactly what I cover this indetail in my free Panic Free TV foundation sequences Its simple sciencebased help forpanic attacks that will show you the fastest, natural direction to go from wherever you areright now back to a life thats as regular, carefree, and panicfree, as anyone elseyou know. The solutions for panic is simple, buttheyre passionately counterintuitive and thats why I initiated this footing line. Again, its totally free, it will makean immediate, important difference in their own lives and to watch it right now, simplyclick on the link on your screen or in the specific characteristics below, enter your details, and get started today on your outing back to a regular, panicfree life Im Michael Norman.Thank you so much better forwatching. Ill see you soon ..
 As found on YouTube
New Explaindio 4 is revolutionary technology which creates fascinating videos by combining 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video. This is why I am extremely excited to be able to tell you that now there is Explaindio 4, which is an easy to use video content creation software that allows you to combine 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video.
As found on YouTube
New Explaindio 4 is revolutionary technology which creates fascinating videos by combining 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video. This is why I am extremely excited to be able to tell you that now there is Explaindio 4, which is an easy to use video content creation software that allows you to combine 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video.
As found on YouTube
New Explaindio 4 is revolutionary technology which creates fascinating videos by combining 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video. This is why I am extremely excited to be able to tell you that now there is Explaindio 4, which is an easy to use video content creation software that allows you to combine 2D & 3D animations, whiteboard sketch elements, and full motion video, all into one powerful, attention grabbing video. 
What can trigger an anxiety attack?
Sometimes it can be easy to find a trigger.For speciman, people with a specific phobia of something can have anxiety when they seethat special object. In some clients, it’s much harder to find a prompt. Panic attacks, for instance, can come out of the blue without any self-evident initiation. Sometimes, people can also experience anticipatory anxiety, so they feel anxious even before they’re in a placewhere they are stressed. In status such as PTSD( posttraumatic stress malady) distres can start after people witness something that prompts them of the past agonizing event.This meaning that the damage has not been fully processed and still feigns people. It’s important to remember that sometimes you can manage anxiety by avoiding the initiations. So, escape establishes it harder to identify a particular trigger ..
As found on YouTube
Guided Imagery for School Anxiety-Social Anxiety Treatment-Anxiety Skills #15
Hi, I’m Emma McAdam, a licensed therapist, in this little Nugget of Help we’re going to apply some tools from adoption and commitment regiman to help with school and social anxiety. This activity is meant to help build an increased ability to face anxiety eliciting status like institution or social locates The purpose of this activity is not relaxation but resilience meaning the ability to experience uncomfortable perceptions with strong empathy and pacify. So during this activity You may feel a couple of spirits, some comfortable and some unpleasant Please stick with the activity through the end and I predict you’ll develop a greater ability to experience your excitements without them limiting you So first check in with yourself, a be engaged in a comfortable locate close your eyes and Take a depth breath Let it out gradually Take a moment and notice your feet wiggle them Now, press them against the floor.Just feel what the flooring feels like pressing back up against your feet Now move your awareness up your legs clench your calves and then soften those muscles Then clench the big-hearted muscles in your thighs for a moment Now relax them and breathe in and breathe out Now move your awareness up to your belly You may feel some hostility here and that’s okay Pretend you’re scientist who has never noticed what that feeling is like Explore that feeling in your stomach and describe it in your psyche. What does it definitely sounds like? Allow it happening there while clenching your stomach muscles as tightly as you can Now breathe out and then take a big inhale Expand your stomach out as far as it becomes Hold that gulp and notice what that feels like Let that air out and move your awareness up to your chest and back Tense, those muscles attract your shoulders up to your ears and hamper them there tightly, clenched hard Then softened those muscles and breathe out gradually Now clench your biceps your upper arms and then liberate Now clench your fists and liberate Move your awareness up to your face and seize your face muscles tightly And now lightened those muscles in your face Now we’re going to do a speedy check of your bodily awareness, what do you notice in your figure? There might be some places in your organization that feel warm soft and comfortable notice those And there might be some residence that feel tighten or pain notice these areas You don’t need to label these even worse or be discouraged, but merely notice them Notice yourself breathing what does it feel like to breathe? Take one more deep breath in and give away very slowly What feelings or sensations are you knowing right now? Some of them may be painful and that’s okay Just notice them, be curious.What does it feel like to feel those sentiments without needing to escape them? Send each of your feelings a bit mental hug. It’s okay to have feelings. Notice if there are any more spirits, perhaps quieter emotions that “youre gonna” feeling too what else are you noticing? Be puzzled. You don’t need them “re going away”. You can treat feeling them. How would you describe each of these sentiments? Take one more deep breath and notice yourself breathing Now let’s envisage yourself going to the first day of clas The bus pushes up to the front of the school and as you get off the bus you feel your gut tighten a bit Perhaps you feel a lot of energy coursing through your torso You may feel a little tense or jumpy and that’s okay It’s perfectly normal to be having these feelings and superstars Most of the other adolescents are feeling a little anxious and aroused extremely You can administer feeling this action Anxiety and fervor are the same physiological response in our body Both of them prepping us for action to perform well, and it’s okay to have this feeling in your person Your old-time habitual suppose is I need to escape or I can’t handle feeling this way But now you remind yourself I can administer feeling this course and be okay.I Don’t need my agitations to go away for me to be alright, I can feel them and notice them and While they are uncomfortable, they can’t trauma me. I is in fact safe in this moment You look around and remember that probably most of the other children are also feeling a little watchful or stimulated right now It’s perfectly natural to feel this way, and it’s not going to harm you You alter your attention back to your breathing and as you step toward the school you notice something beautiful What is it? Perhaps the clear sky or the light-green grass Take a time and notice that one pretty thing You hear lots of adolescents are running noisily toward the school some are meeting up with their friends some are alone suddenly you were supposed to meditated What if no one will be my friend? or You worry that people are looking at you in a funny way.For a moment You have visions of a catastrophe run through your psyche. You’re afraid of being rejected being alone being a loser But you rapidly notice those remembers they are distressing and loudly judges, but they are just supposes Just as you can notice yourself listening to my expression at this moment. You can notice yourself having those designs They aren’t truthful They don’t help you be the person that you appreciate Because you appraise being style, you be concerned about connecting with people You want to be a good friend. You can act on those qualities and good things will happen People will want to be friends with you when they get to know you because of who you are You notice those frightening thoughts and you imagine them written on the side of the bus and the bus begins to pull away You remember that you’re okay You have some inner endowments to share with the world. Even if you are quiet or observant instead of a thundering idiot. Take a time and think of one of the talents that you have One thing that you are good at like has become a good listener or noticing others needs for example You remember some of the people who love you and looks just like you, your friends your parents You remember that you are safe right now.It may feel uncomfortable But you can handle that You may feel a bit of distres But you can open up some opening for that suspicion inside of you. You don’t need to represent that nervousnes go away to be okay. Imagine that your anxiety is a little child saying What if no one likes me? and you say Come now little tension. I want to give you a hug See it’s awkward, but you can experience it and it doesn’t trauma you. You walk through the figurehead entrances of the school and there’s a lot of noise and commotion Not your favorite So you thoughts over to your locker, You previously know where it is because you went to the open live And you open your locker and a gentle float of your favorite flavor comes out of it You waste a minute.Just bask that fragrance Breathe in deeply Now you walk to your first class, you know Right where it is and you arrive a few minutes early you take your seat and look around There’s a few other adolescents sitting down and you say hi to the girl sitting next to you She says hi back, and then suddenly you feel so awkward You start worrying that you should have said more or maybe you shouldn’t have said anything or that maybe you didn’t determine fairly nose contact and unexpectedly you’re hyper aware of how you’re sitting in your chair and you can feel Your heart thrashing a little faster and your hands sweating a little bit and then you notice yourself Tensing up a little and you can notice your thoughts Now in this moment notice what’s going on in your person and in your mind.You retain what your mentor said you don’t actually act tricky you only feel clumsy No one else has even paying attention to you. They’re all anxious and elicited about their first day of school And they’re too busy worrying about what parties “ve been thinking about” them to notice you You can still feel that tight feeling in your tummy and your sweaty palms and you tell yourself.That’s ok It’s ok to have uncomfortable perceptions sometimes. I can let myself feel this experience without needing to escape it or make it go away You know that it never helps to beat yourself up so instead you precisely testify yourself a little compassion You going to go to noticing for a while and you sifted through your experience in this moment. So Sift is an acronym S is for agitations Notice your physical perceptions precisely notice them both cozy and disagreeable. I is for epitomes What do you envisage in this moment? Can you notice those portraits and then bring yourself back to center with the wheeze? Can you notice those portraits in your manager And then bring yourself back to center by acknowledge your wheeze F is for feelings, what ardours are you knowledge? Are you having more than one? What is one thing you’re elicited about And the T is thoughts Notice, what are you thinking? You don’t need to duel or change your thoughts. Just notice yourself having them You take another deep gulp and you’re feeling kind of proud That right now you’re experiencing a little anxiety But you’re okay with it It’s a little embarrassing But you’re beginning to develop the skill of letting yourself feel it You give yourself a little imaginary pat on the back for being indomitable For letting yourself do hard things and feel hard things and stick with it The bell sounds and the coach starts class he goes through the roll.You Pay close attention waiting for him to call your name.And then when he does you say here and Maybe you wonder a little if you did, okay, but no one even looks at you They’re all exactly paying attention to their own stuff right now You remind yourself that you can do hard things You take another deep gulp and tell it out gradually Then the teacher extends out a sheet of paper to everyone on it is an icebreaker activity You detest these. you have to go around the room and find someone who has broken their arm and someone who’s lived in another state and someone who Has a baby reptile Maybe you’re afraid that you’ll be awkward You might worry that no one will ask you questions or that you’re afraid that people will ask you questions You press your feet into the floor feeling the flooring pulping back up at you You notice your panic It’s telling you to run away, to avoid, to hide to be silent and you notice that fear You be recognized, you say hello fear.I’ve noticed you’re trying to hang out with me today I know I can’t meet you go away But you’re not the boss of me and I still get to decide what matters to me so fear You can restrain constructing suggestions, but I know what’s more important You is a well-known fact that you don’t like these icebreaker works But you also know that you wishes to be oblige some friends and you don’t want to isolate yourself on the first day So you look around and consider another minor who seems kind of hushed and is standing by himself You walk over to him and you feel a little awkward, but you don’t actually seem touchy from the outside. You look perfectly normal When you get to his desk, you look down at your article and you ask him.What’s your favorite notebook? He seems a little shy so you been listening while he says you about the book series that he likes then he looks at his paper and asks you What’s your favorite journal? You tell him about your favorite work and what you like about it and you can see in his smile that he’s speak that one And he likes it extremely. He must be a special type of nerd like you You stand around and other adolescents comes down to you and ask their questions you ask yours and pretty soon your newspapers all filled out The teacher gets back up. He seems nice and also a little funny and you think you’ll like his class The rest of that class leads somewhat smoothly you only sit in your chair and predict the syllabus while the educator tells you the class Rules and talks about what you’re going to learn so far so good You feel proud of yourself after your first day of clas There were hours “thats been” awkward, but that’s okay and there were experiences that were good You learned more about what to expect and although you felt some anxiety.You didn’t let it boss you around You were gentle with yourself Patient with your sentiments and whizs and you two are heroic to show up and feel lots of things today Excitement beauty anxiety hope for new friends and a sense of confidence in your ability to do hard-bitten things Now come back to the present moment Notice your feet on the floor notice your wheeze Think back over this exercise Was it unpleasant at times? But you fastened with it.You chose to do something challenging because something else mattered more than avoidance Take a deep breath and give yourself a little pat on the back for letting yourself experience your passions You are on the pathway to growth an emotional strong Keep up the good work.

As found on YouTube